

Low grade inflammation and coronary heart disease: prospective study and updated meta-analyses
- PMID: 10903648
- PMCID: PMC27435
- DOI: 10.1136/bmj.321.7255.199
Low grade inflammation and coronary heart disease: prospective study and updated meta-analyses
Abstract
Objective: To assess associations between baseline values of four different circulating markers of inflammation and future risk of coronary heart disease, potential triggers of systemic inflammation (such as persistent infection), and other markers of inflammation.
Design: Nested case-control comparisons in a prospective, population based cohort.
Setting: General practices in 18 towns in Britain.
Participants: 506 men who died from coronary heart disease or had a non-fatal myocardial infarction and 1025 men who remained free of such disease until 1996 selected from 5661 men aged 40-59 years who provided blood samples in 1978-1980.
Main outcome measures: Plasma concentrations of C reactive protein, serum amyloid A protein, and serum albumin and leucocyte count. Information on fatal and non-fatal coronary heart disease was obtained from medical records and death certificates.
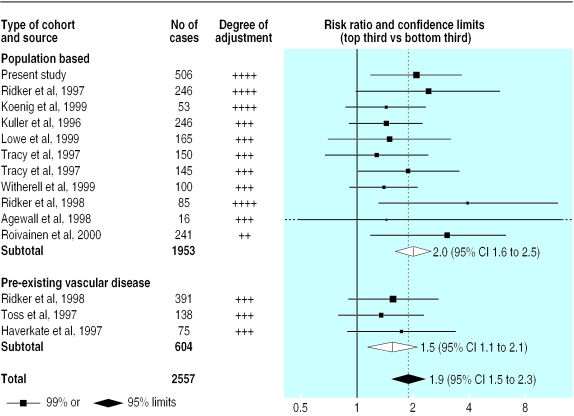
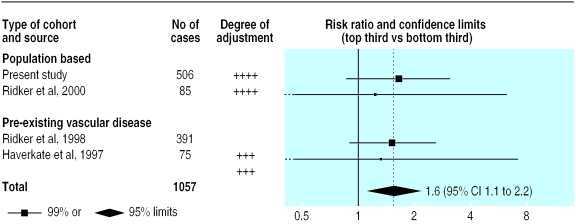
Results: Compared with men in the bottom third of baseline measurements of C reactive protein, men in the top third had an odds ratio for coronary heart disease of 2.13 (95% confidence interval 1.38 to 3.28) after age, town, smoking, vascular risk factors, and indicators of socioeconomic status were adjusted for. Similar adjusted odds ratios were 1.65 (1.07 to 2.55) for serum amyloid A protein; 1.12 (0.71 to 1.77) for leucocyte count; and 0.67 (0.43 to 1.04) for albumin. No strong associations were observed of these factors with Helicobacter pylori seropositivity, Chlamydia pneumoniae IgG titres, or plasma total homocysteine concentrations. Baseline values of the acute phase reactants were significantly associated with one another (P<0.0001), although the association between low serum albumin concentration and leucocyte count was weaker (P=0.08).
Conclusion: In the context of results from other relevant studies these findings suggest that some inflammatory processes, unrelated to the chronic infections studied here, are likely to be involved in coronary heart disease.
Figures
Comment in
-
Heart disease and the inflammatory response.BMJ. 2000 Jul 22;321(7255):187-8. doi: 10.1136/bmj.321.7255.187. BMJ. 2000. PMID: 10903629 Free PMC article. No abstract available.
References
-
- Pepys MB, Baltz ML. Acute phase proteins with special reference to C-reactive and related proteins (pentaxins) and serum amyloid A protein. Adv Immun. 1983;34:141–212. - PubMed
-
- Danesh J, Collins R, Appleby P, Peto R. Fibrinogen, C-reactive protein, albumin or white cell count: meta-analyses of prospective studies of coronary heart disease. JAMA. 1998;279:1477–1482. - PubMed
-
- Ridker PM, Rifai N, Pfeffer MA, Sacks FM, Braunwald E. Long-term effects of pravastatin on plasma concentration of C-reactive protein. Circulation. 1999;100:230–235. - PubMed
-
- Wilkins J, Gallimore JR, Moore EG, Pepys MB. Rapid automated high sensitivity enzyme immunoassay of C-reactive protein. Clin Chem. 1998;44:1358–1361. - PubMed
-
- Wilkins J, Gallimore JR, Tennent GA, Hawkins PN, Limburg PC, van Rijswijk MH, et al. Rapid automated enzyme immunoassay of serum amyloid A. Clin Chem. 1994;40:1284–1290. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials