

Problematic pigmented lesions: approach to diagnosis
- PMID: 10911797
- PMCID: PMC1731214
- DOI: 10.1136/jcp.53.6.409
Problematic pigmented lesions: approach to diagnosis
Abstract
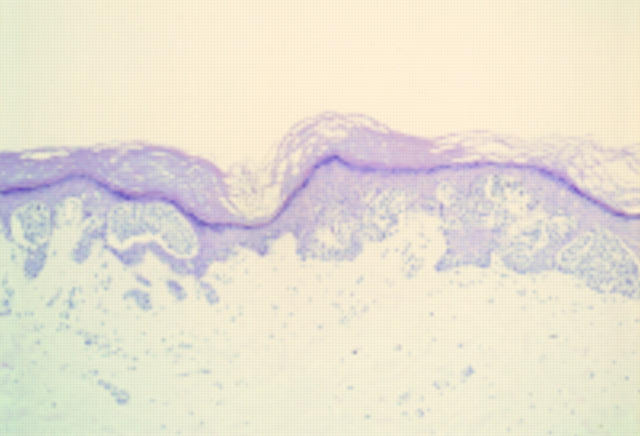
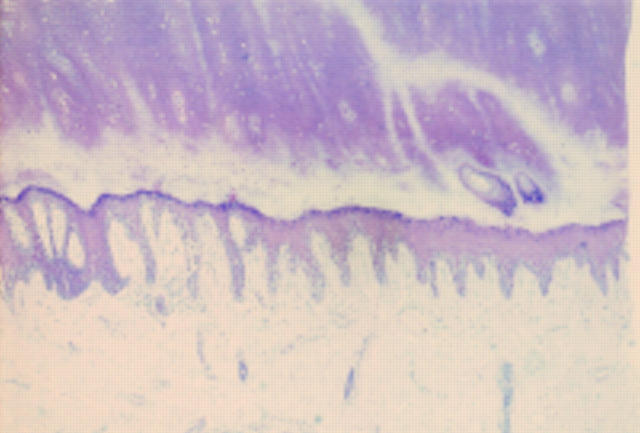
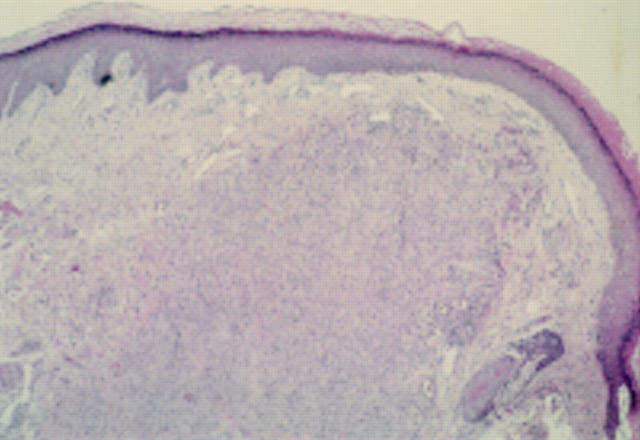
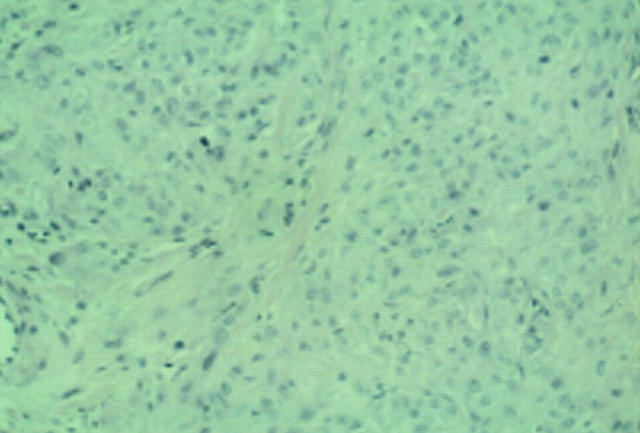
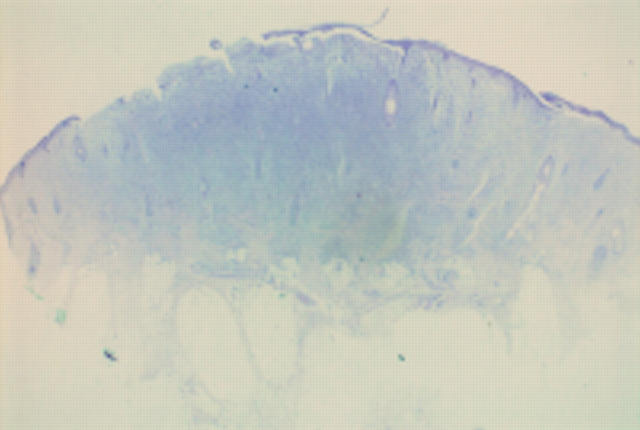
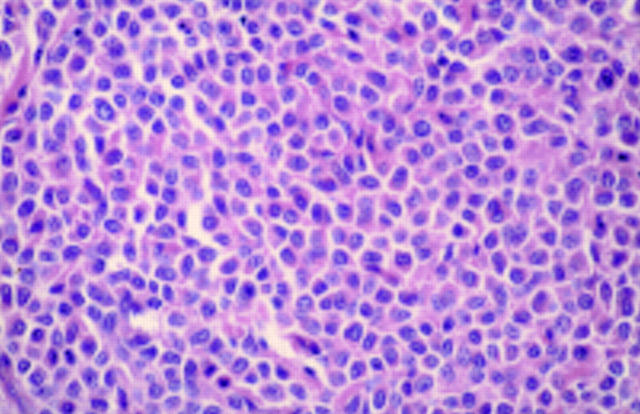
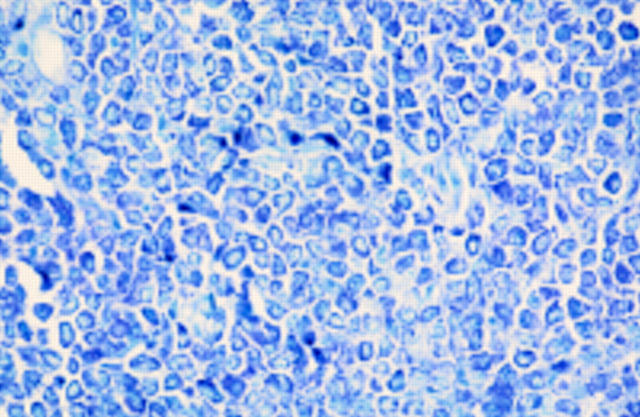
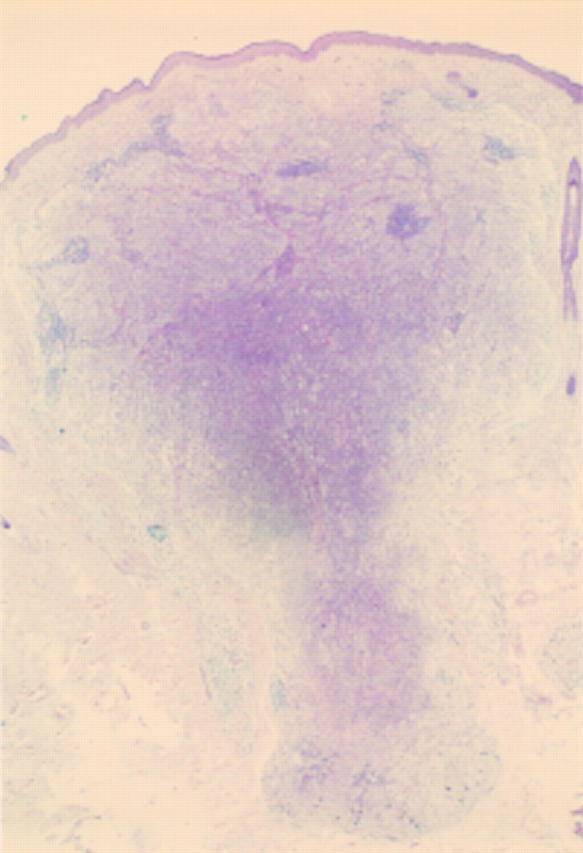
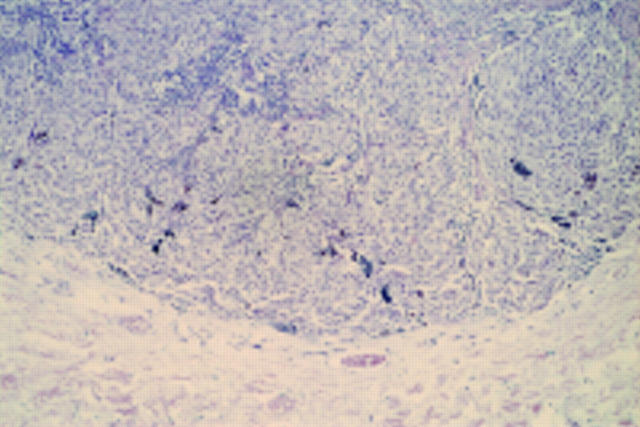
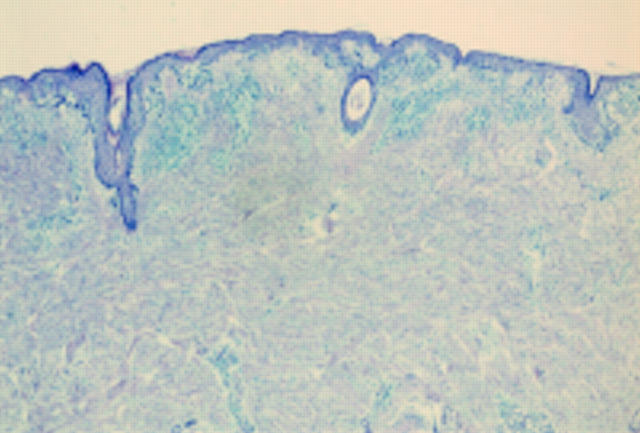
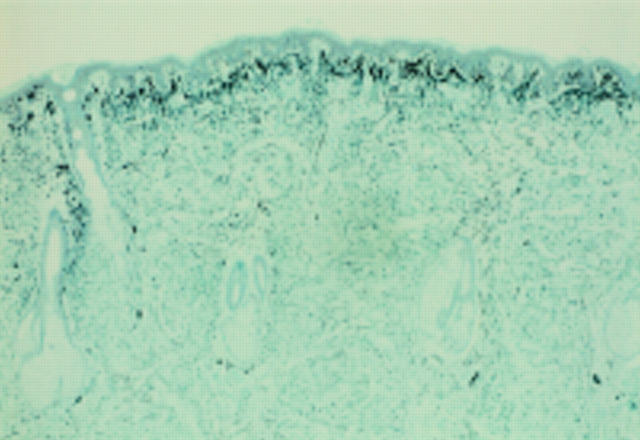
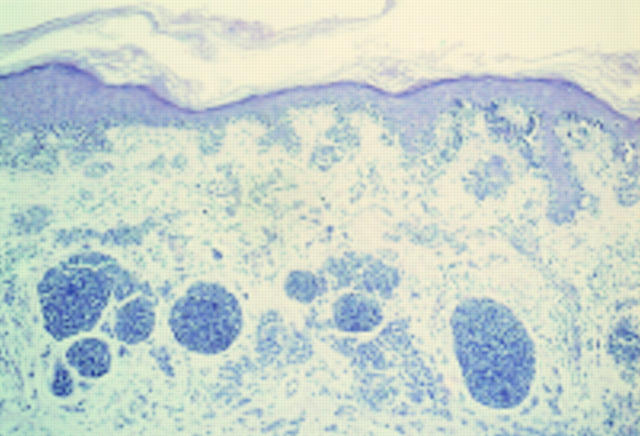
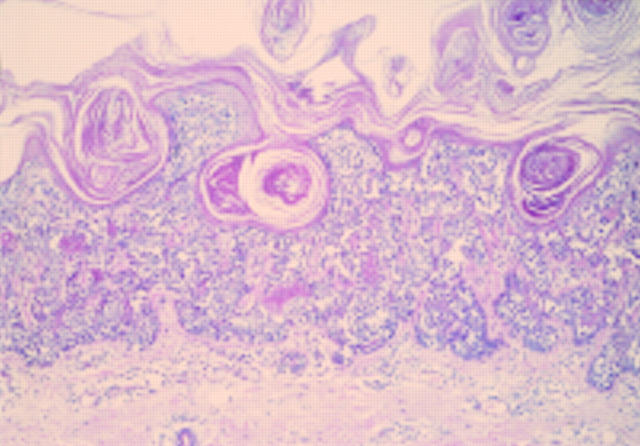
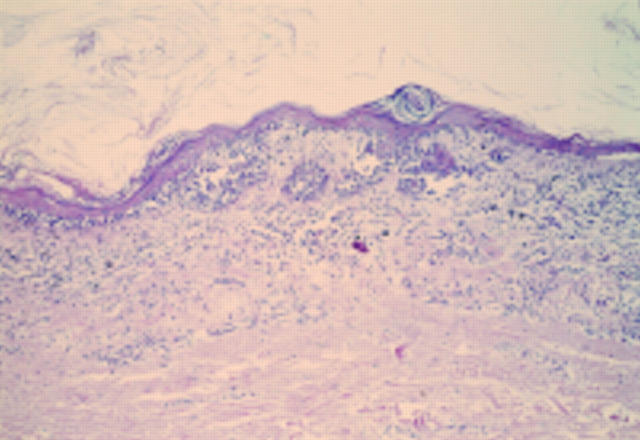
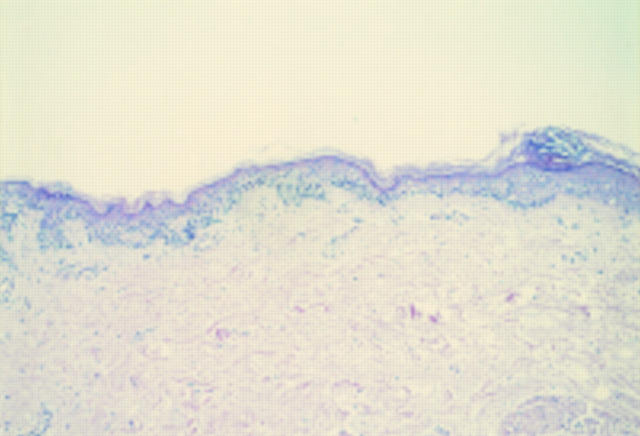
A number of pigmented lesions are difficult to classify and raise the possibility of a melanoma diagnosis. Care should be exercised to exclude non-melanocytic lesions, and benign melanocytic entities, both of which can mimic melanoma histologically. In addition, the possibility of the lesion being a melanoma variant or epidermotropic metastasis should be considered. There will still be some cases that are difficult to resolve. These usually fall into one of three categories: atypical junctional melanocytic lesion versus early melanoma; naevus versus naevoid melanoma; and atypical Spitz, cellular blue, and deep penetrating naevi versus thick melanoma. These will pose problems even for experts. The atypical Spitz lesions are perhaps the most important category because they tend to be from younger individuals, the differential diagnosis is thick melanoma, and there is no single discriminating histological feature.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical