

Laparoscopic removal of a perforated intrauterine device from the perirectal fat
- PMID: 10917124
- PMCID: PMC3015382
Laparoscopic removal of a perforated intrauterine device from the perirectal fat
Abstract
Background: The intrauterine device (IUD) was a very common form of birth control in the United States. The most serious potential complication of IUD use is uterine perforation. Uterine perforation is common among women with "lost" IUDs and can cause severe morbidity and mortality and should be carefully managed. The recommended treatment is removal of the perforating IUD. This can usually be managed laparoscopically unless bowel perforation or other severe sepsis is present.
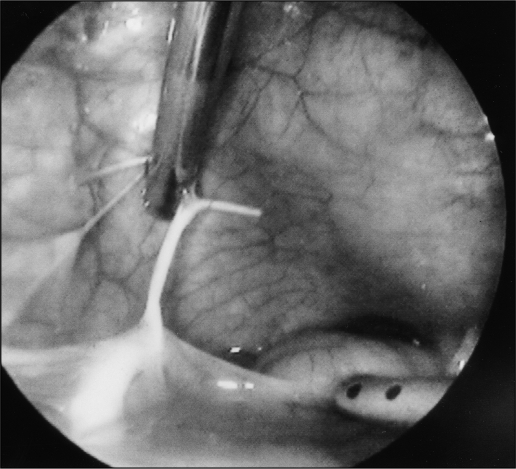
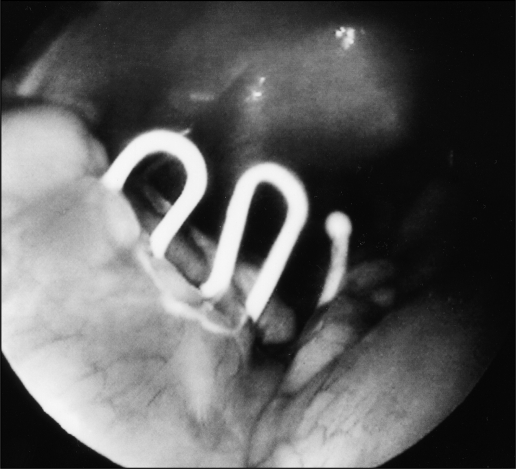
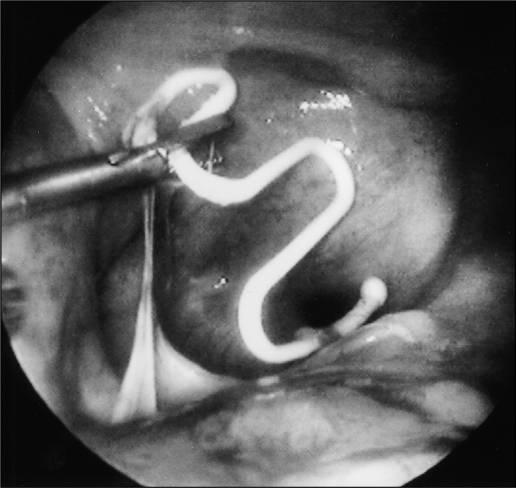
Methods: An intra-abdominal IUD was removed laparoscopically from the perirectal fat of a 49-year-old woman who had been diagnosed over 20 years earlier with an "expelled" IUD.
Conclusions: It is important that the possibility of uterine perforation be considered in anyone who has had a diagnosis of an expelled IUD without actual confirmation that the IUD is no longer present in the body. In any woman who presents with pelvic pain and a history of a "lost" IUD, the surgeon should have a high index of suspicion and obtain radiological studies. It may be advisable to question women about possible IUD use when they present with pelvic pain of unknown origin.
Figures
Similar articles
-
Uterine perforation caused by intrauterine devices: clinical course and treatment.Hum Reprod. 2013 Jun;28(6):1546-51. doi: 10.1093/humrep/det074. Epub 2013 Mar 22. Hum Reprod. 2013. PMID: 23526304
-
A lost intrauterine device. Guess where we found it and how it happened?Eur J Contracept Reprod Health Care. 2006 Mar;11(1):47-9. doi: 10.1080/13625180500456791. Eur J Contracept Reprod Health Care. 2006. PMID: 16546816
-
The management of intrauterine devices following uterine perforation.Contraception. 1991 Jan;43(1):77-81. doi: 10.1016/0010-7824(91)90128-3. Contraception. 1991. PMID: 1825971
-
Complete and partial uterine perforation and embedding following insertion of intrauterine devices. II. Diagnostic methods, prevention, and management.Obstet Gynecol Surv. 1981 Aug;36(8):401-17. doi: 10.1097/00006254-198108000-00001. Obstet Gynecol Surv. 1981. PMID: 6455610 Review.
-
Perforation of the bladder by the intrauterine device.Obstet Gynecol Surv. 1984 Feb;39(2):59-66. doi: 10.1097/00006254-198402000-00001. Obstet Gynecol Surv. 1984. PMID: 6229704 Review.
Cited by
-
Intrauterine contraceptive device migration presenting as abdominal wall swelling: a case report.Case Rep Surg. 2011;2011:305914. doi: 10.1155/2011/305914. Epub 2011 Oct 19. Case Rep Surg. 2011. PMID: 22606574 Free PMC article.
-
Laparoscopic removal of an intrauterine device following colon perforation.JSLS. 2010 Jul-Sep;14(3):456-8. doi: 10.4293/108680810X12924466006963. JSLS. 2010. PMID: 21333210 Free PMC article.
-
Intracorporeal suturing and knot tying broadens the clinical applicability of laparoscopy.JSLS. 2003 Apr-Jun;7(2):137-40. JSLS. 2003. PMID: 12856844 Free PMC article.
-
Benefit-risk assessment of the levonorgestrel intrauterine system in contraception.Drug Saf. 2004;27(15):1185-204. doi: 10.2165/00002018-200427150-00003. Drug Saf. 2004. PMID: 15588115
-
Intrauterine devices and risk of uterine perforation: current perspectives.Open Access J Contracept. 2016 Mar 16;7:19-32. doi: 10.2147/OAJC.S85546. eCollection 2016. Open Access J Contracept. 2016. PMID: 29386934 Free PMC article. Review.
References
-
- Mishell DR., Jr Intrauterine devices: mechanisms of action, safety, and efficacy. Contraception. 1998;58:45S–53S - PubMed
-
- Zimmer DF., Jr Avoiding litigation in a new age of IUDs. Obstet Gynecol Surv. 1996;51(12):56S–60S - PubMed
-
- Andersson K, Ryde-Blomquist E, Lindell K, Odlind V, Milsom I. Perforation with intrauterine devices: report from a Swedish survey. Contraception. 1998;57:251–255 - PubMed
-
- Fortney JA, Feldblum PJ, Raymond EG. Intrauterine devices: the optimal long-term contraceptive method. J Reproductive Med. 1999;44(3):269–274 - PubMed
-
- United Nations Development Programme / United Nations Population Fund / World Health Organization / World Bank, Special Programme of Research Training in Human Reproduction Long-term reversible contraception: twelve years of experience with the TCu380A and TCu220C. Contraception. 1997;56:341–352 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources