

Predictors of progression to cancer in Barrett's esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets
- PMID: 10925966
- PMCID: PMC1783835
- DOI: 10.1111/j.1572-0241.2000.02196.x
Predictors of progression to cancer in Barrett's esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets
Abstract
Objective: Barrett's esophagus develops in 5-20% of patients with gastroesophageal reflux disease and predisposes to esophageal adenocarcinoma. The value of endoscopic biopsy surveillance is questioned because most patients do not develop cancer. Furthermore, observer variation in histological diagnosis makes validation of surveillance guidelines difficult because varying histological interpretations may lead to different estimated rates of progression. Thus, objective biomarkers need to be validated for use with histology to stratify patients according to their risk for progression to cancer.
Methods: We prospectively evaluated patients using a systematic endoscopic biopsy protocol with baseline histological and flow cytometric abnormalities as predictors and cancer as the outcome.
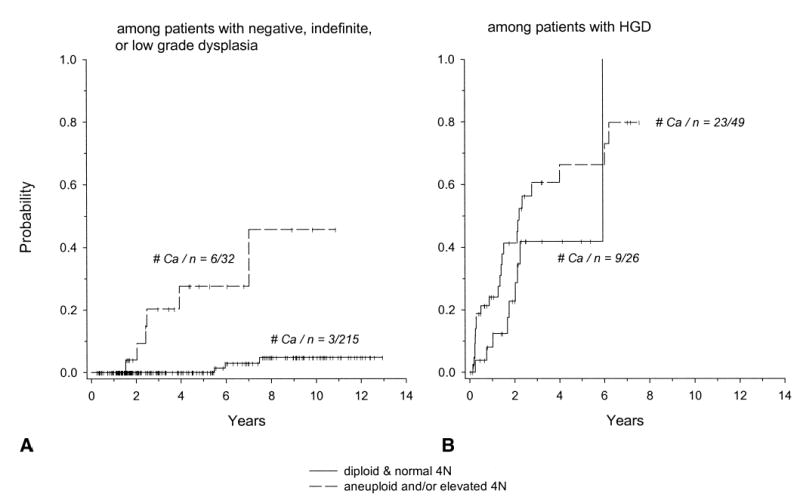
Results: Among patients with negative, indefinite, or low-grade dysplasia, those with neither aneuploidy nor increased 4N fractions had a 0% 5-yr cumulative cancer incidence compared with 28% for those with either aneuploidy or increased 4N. Patients with baseline increased 4N, aneuploidy, and high-grade dysplasia had 5-yr cancer incidences of 56%, 43%, and 59%, respectively. Aneuploidy, increased 4N, or HGD were detected at baseline in all 35 patients who developed cancer within 5 yr.
Conclusions: A systematic baseline endoscopic biopsy protocol using histology and flow cytometry identifies subsets of patients with Barrett's esophagus at low and high risk for progression to cancer. Patients whose baseline biopsies are negative, indefinite, or low-grade displasia without increased 4N or aneuploidy may have surveillance deferred for up to 5 yr. Patients with cytometric abnormalities merit more frequent surveillance, and management of high-grade dysplasia can be individualized.
Figures


References
-
- Locke GR, III, Talley NJ, Fett SL, et al. Prevalence and clinical spectrum of gastroesophageal reflux: A population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112:1448–56. - PubMed
-
- Winters C, Jr, Spurling TJ, Chobanian SJ, et al. Barrett’s esophagus. A prevalent, occult complication of gastroesophageal reflux disease. Gastroenterology. 1987;92:118–24. - PubMed
-
- Spechler SJ, Zeroogian JM, Antonioli DA, et al. Prevalence of metaplasia at the gastro-oesophageal junction. Lancet. 1994;344:1533–6. - PubMed
-
- Reid BJ. Barrett’s esophagus and esophageal adenocarcinoma. In: Roy Wong KH, editor. Gastroenterology Clinics of North America: Mucosal diseases of the esophagus. Philadelphia: WB Saunders; 1991. pp. 817–34. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF., Jr Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83:2049–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
