

Calcium-stimulated insulin secretion in diffuse and focal forms of congenital hyperinsulinism
- PMID: 10931418
- PMCID: PMC4151173
- DOI: 10.1067/mpd.2000.107386
Calcium-stimulated insulin secretion in diffuse and focal forms of congenital hyperinsulinism
Abstract
Objectives: To identify infants with hyperinsulinism caused by defects of the beta-cell adenosine triphosphate-dependent potassium channel complex and to distinguish focal and diffuse forms of hyperinsulinism caused by these mutations.
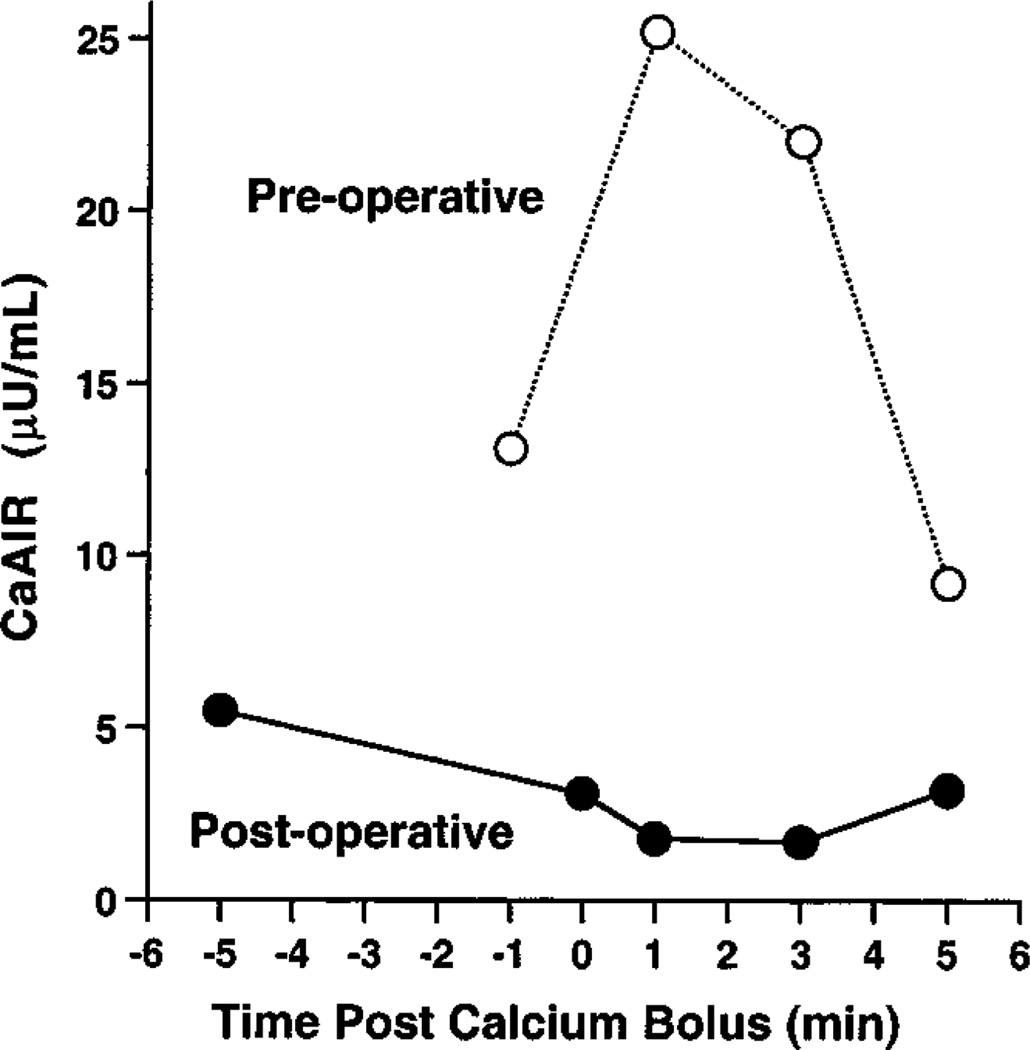
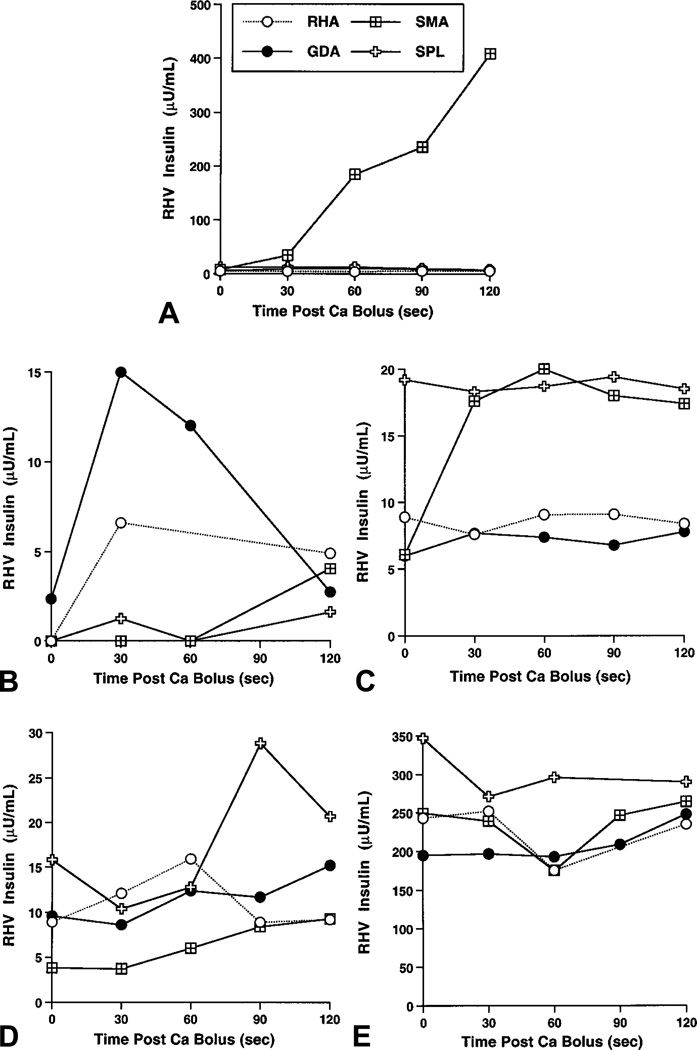
Study design: The acute insulin response to intravenous calcium stimulation (CaAIR) was determined in 9 patients <20 years with diffuse hyperinsulinism caused by defective beta-cell sulfonylurea receptor (SUR1(-/-)), 3 patients with focal congenital hyperinsulinism (6 weeks to 18 months), a 10-year-old with insulinoma, 5 with hyperinsulinism/hyperammonemia syndrome caused by defective glutamate dehydrogenase (6 months to 28 years), 4 SUR1(+/-) heterozygotes with no symptoms, and 9 normal adults. Three infants with congenital focal disease, 1 with diffuse hyperinsulinism, and the child with insulinoma underwent selective pancreatic intra-arterial calcium stimulation with hepatic venous sampling.
Results: Children with diffuse SUR1(-/-) disease and infants with congenital focal hyperinsulinism responded to CaAIR, whereas the normal control group, patients with hyperinsulinism/hyperammonemia syndrome, and SUR1(+/-) carriers did not. Selective arterial calcium stimulation of the pancreas with hepatic venous sampling revealed selective, significant step-ups in insulin secretion that correlated anatomically with the location of solitary lesions confirmed surgically in 2 of 3 infants with congenital focal disease and in the child with insulinoma. Selective arterial calcium stimulation of the pancreas with hepatic venous sampling demonstrated markedly elevated baseline insulin levels throughout the pancreas of the infant with diffuse hyperinsulinism.
Conclusions: The intravenous CaAIR is a safe and simple test for identifying infants with diffuse SUR1(-/-) hyperinsulinism or with focal congenital hyperinsulinism. Preoperative selective arterial calcium stimulation of the pancreas with hepatic venous sampling can localize focal lesions causing hyperinsulinism in children. The combination of these calcium stimulation tests may help distinguish focal lesions suitable for cure by local surgical resection.
Figures
Similar articles
-
Preoperative evaluation of infants with focal or diffuse congenital hyperinsulinism by intravenous acute insulin response tests and selective pancreatic arterial calcium stimulation.J Clin Endocrinol Metab. 2004 Jan;89(1):288-96. doi: 10.1210/jc.2003-030965. J Clin Endocrinol Metab. 2004. PMID: 14715863
-
Dysregulation of insulin secretion in children with congenital hyperinsulinism due to sulfonylurea receptor mutations.Diabetes. 2001 Feb;50(2):322-8. doi: 10.2337/diabetes.50.2.322. Diabetes. 2001. PMID: 11272143 Free PMC article.
-
Genotype-phenotype correlations in children with congenital hyperinsulinism due to recessive mutations of the adenosine triphosphate-sensitive potassium channel genes.J Clin Endocrinol Metab. 2005 Feb;90(2):789-94. doi: 10.1210/jc.2004-1604. Epub 2004 Nov 23. J Clin Endocrinol Metab. 2005. PMID: 15562009
-
[Congenital hyperinsulinism in newborn and infant].Arch Pediatr. 2005 Nov;12(11):1628-35. doi: 10.1016/j.arcped.2005.07.016. Epub 2005 Sep 28. Arch Pediatr. 2005. PMID: 16198094 Review. French.
-
Molecular mechanisms of neonatal hyperinsulinism.Horm Res. 2006;66(6):289-96. doi: 10.1159/000095938. Epub 2006 Sep 26. Horm Res. 2006. PMID: 17003566 Review.
Cited by
-
Clinical practice guidelines for congenital hyperinsulinism.Clin Pediatr Endocrinol. 2017;26(3):127-152. doi: 10.1297/cpe.26.127. Epub 2017 Jul 27. Clin Pediatr Endocrinol. 2017. PMID: 28804205 Free PMC article.
-
Congenital Hyperinsulinism in China: A Review of Chinese Literature Over the Past 15 Years.J Clin Res Pediatr Endocrinol. 2017 Sep 1;9(3):194-201. doi: 10.4274/jcrpe.3934. Epub 2017 Mar 8. J Clin Res Pediatr Endocrinol. 2017. PMID: 28270372 Free PMC article. Review.
-
Surgical treatment of congenital hyperinsulinism: Results from 500 pancreatectomies in neonates and children.J Pediatr Surg. 2019 Jan;54(1):27-32. doi: 10.1016/j.jpedsurg.2018.10.030. Epub 2018 Oct 5. J Pediatr Surg. 2019. PMID: 30343978 Free PMC article.
-
Role of 18F-DOPA PET/CT imaging in congenital hyperinsulinism.Rev Endocr Metab Disord. 2010 Sep;11(3):165-9. doi: 10.1007/s11154-010-9145-1. Rev Endocr Metab Disord. 2010. PMID: 20878481 Review.
-
Persistent hyperinsulinemic hypoglycemia of infancy: An overview of current concepts.J Indian Assoc Pediatr Surg. 2012 Jul;17(3):99-103. doi: 10.4103/0971-9261.98119. J Indian Assoc Pediatr Surg. 2012. PMID: 22869973 Free PMC article.
References
-
- Stanley CA. Hyperinsulinism in infants and children. Pediatr Clin North Am. 1997;44:363–374. - PubMed
-
- Aguilar-Bryan L, Bryan J. Molecular biology of adenosine triphosphate-sensitive potassium channels. Endocr Rev. 1999;20:101–135. - PubMed
-
- Thomas P, Ye YY, Lightner E. Mutations of the pancreatic islet inward rectifier KIR6.2 also leads to familial persistent hyperinsulinemic hypoglycemia of infancy. Hum Mol Genet. 1996;5:1809–1812. - PubMed
-
- Nestorowicz A, Inagaki N, Gonoi T, Schoor KP, Wilson BA, Glaser B, et al. A nonsense mutation in the inward rectifier potassium channel gene, Kir6.2, is associated with familial hyperinsulinism. Diabetes. 1997;46:1743–1748. - PubMed
-
- Glaser B, Kesavan P, Heyman M, Davis E, Cuesta A, Buchs A, et al. Familial hyperinsulinism caused by an activating glucokinase mutation. N Engl J Med. 1998;338:226–230. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
