

Three-dimensional magnetic resonance spectroscopic imaging of brain and prostate cancer
- PMID: 10933075
- PMCID: PMC1531872
- DOI: 10.1038/sj.neo.7900081
Three-dimensional magnetic resonance spectroscopic imaging of brain and prostate cancer
Abstract
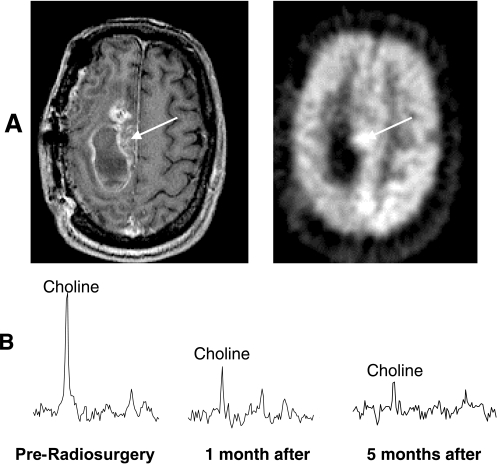
Clinical applications of magnetic resonance spectroscopic imaging (MRSI) for the study of brain and prostate cancer have expanded significantly over the past 10 years. Proton MRSI studies of the brain and prostate have demonstrated the feasibility of noninvasively assessing human cancers based on metabolite levels before and after therapy in a clinically reasonable amount of time. MRSI provides a unique biochemical "window" to study cellular metabolism noninvasively. MRSI studies have demonstrated dramatic spectral differences between normal brain tissue (low choline and high N-acetyl aspartate, NAA) and prostate (low choline and high citrate) compared to brain (low NAA, high choline) and prostate (low citrate, high choline) tumors. The presence of edema and necrosis in both the prostate and brain was reflected by a reduction of the intensity of all resonances due to reduced cell density. MRSI was able to discriminate necrosis (absence of all metabolites, except lipids and lactate) from viable normal tissue and cancer following therapy. The results of current MRSI studies also provide evidence that the magnitude of metabolic changes in regions of cancer before therapy as well as the magnitude and time course of metabolic changes after therapy can improve our understanding of cancer aggressiveness and mechanisms of therapeutic response. Clinically, combined MRI/MRSI has already demonstrated the potential for improved diagnosis, staging and treatment planning of brain and prostate cancer. Additionally, studies are under way to determine the accuracy of anatomic and metabolic parameters in providing an objective quantitative basis for assessing disease progression and response to therapy.
Figures













References
-
- Arnold DL, Shoubridge EA, Feindel W, Villemure JG. Metabolic changes in cerebral gliomas within hours of treatment with intra-arterial BCNU demonstrated by phosphorus magnetic resonance spectroscopy. Can J Neurol Sci. 1987;14:570–575. - PubMed
-
- Arnold DL, Shoubridge EA, Emrich J, Feindel W, Villemure JG. Early metabolic changes following chemotherapy of human gliomas in vivo demonstrated by phosphorus magnetic resonance spectroscopy. Invest Radiol. 1989;24:958–961. - PubMed
-
- Arnold DL, Shoubridge EA, Villemure JG, Feindel W. Proton and phosphorus magnetic resonance spectroscopy of human astrocytomas in vivo. Preliminary observations on tumor grading. NMR Biomed. 1990;3:184–189. - PubMed
-
- Arnold DL, Emrich JF, Shoubridge EA, Villemure JG, Feindel W. Characterization of astrocytomas, meningiomas, and pituitary adenomas by phosphorus magnetic resonance spectroscopy. J Neurosurg. 1991;74:447–453. - PubMed
-
- Arnold DL, De Stefano N. Magnetic resonance spectroscopy in vivo: applications in neurological disorders. Ital J Neurol Sci. 1997;18:321–329. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous