

Human immunodeficiency virus type 1 mutations selected in patients failing efavirenz combination therapy
- PMID: 10952598
- PMCID: PMC90088
- DOI: 10.1128/AAC.44.9.2475-2484.2000
Human immunodeficiency virus type 1 mutations selected in patients failing efavirenz combination therapy
Abstract
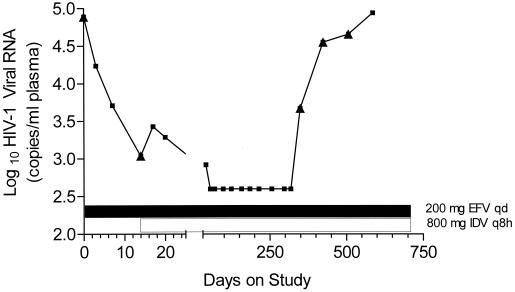
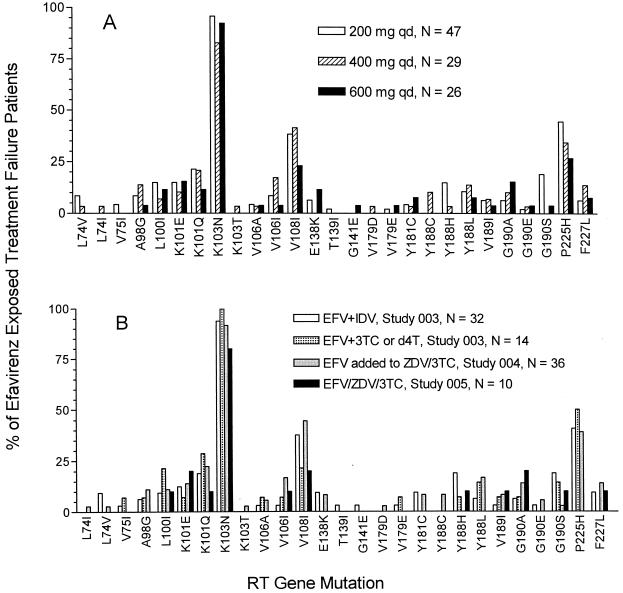
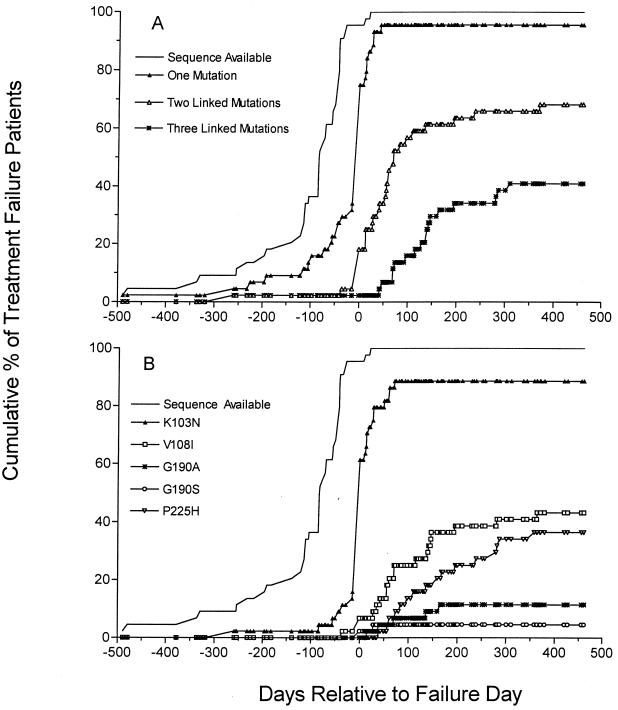
Efavirenz is a potent and selective nonnucleoside inhibitor of human immunodeficiency virus type 1 (HIV-1) reverse transcriptase (RT). Nucleotide sequence analyses of the protease and RT genes (coding region for amino acids 1 to 229) of multiple cloned HIV-1 genomes from virus found in the plasma of patients in phase II clinical studies of efavirenz combination therapy were undertaken in order to identify the spectrum of mutations in plasma-borne HIV-1 associated with virological treatment failure. A K103N substitution was the HIV-1 RT gene mutation most frequently observed among plasma samples from patients for whom combination therapy including efavirenz failed, occurring in at least 90% of cases of efavirenz-indinavir or efavirenz-zidovudine (ZDV)-lamivudine (3TC) treatment failure. V108I and P225H mutations were observed frequently, predominantly in viral genomes that also contained other nonnucleoside RT inhibitor (NNRTI) resistance mutations. L100I, K101E, K101Q, Y188H, Y188L, G190S, G190A, and G190E mutations were also observed. V106A, Y181C, and Y188C mutations, which have been associated with high levels of resistance to other NNRTIs, were rare in the patient samples in this study, both before and after exposure to efavirenz. The spectrum of mutations observed in cases of virological treatment failure was similar for patients initially dosed with efavirenz at 200, 400, or 600 mg once a day and for patients treated with efavirenz in combination with indinavir, stavudine, or ZDV-3TC. The proportion of patients carrying NNRTI resistance mutations, usually K103N, increased dramatically at the time of initial viral load rebound in cases of treatment failure after exposure to efavirenz. Viruses with multiple, linked NNRTI mutations, especially K103N-V108I and K103N-P225H double mutants, accumulated more slowly following the emergence of K103N mutant viruses.
Figures
References
-
- Altschul S F, Gish W, Miller W, Myers E W, Lipman D J. Basic local alignment search tool. J Mol Biol. 1990;215:403–410. - PubMed
-
- Balzarini J, Pelemans H, Esnouf R, De Clercq E. A novel mutation (F227L) arises in the reverse transcriptase of human immunodeficiency virus type 1 on dose-escalating treatment of HIV type 1-infected cell cultures with the nonnucleoside reverse transcriptase inhibitor thiocarboxanilide UC-781. AIDS Res Hum Retrovir. 1998;14:255–260. - PubMed
-
- Birnboim H C. A rapid alkaline extraction method for the isolation of plasmid DNA. Methods Enzymol. 1983;100:243–255. - PubMed
-
- Byrnes V W, Sardana V V, Schleif W A, Condra J H, Waterbury J A, Wolfgang J A, Long W J, Schneider C L, Schlabach A J, Wolanski B S. Comprehensive mutant enzyme and viral variant assessment of human immunodeficiency virus type 1 reverse transcriptase resistance to nonnucleoside inhibitors. Antimicrob Agents Chemother. 1993;37:1576–1579. - PMC - PubMed
-
- Carr A, Vella S, de Jong M D, Sorice F, Imrie A, Boucher C A, Cooper D A. Controlled trial of nevirapine plus zidovudine versus zidovudine alone in p24 antigenaemic HIV-infected patients. The Dutch-Italian-Australian Nevirapine Study Group. AIDS. 1996;10:635–641. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
