

Intracranial vertebrobasilar stenosis: angioplasty and follow-up
- PMID: 10954282
- PMCID: PMC8174918
Intracranial vertebrobasilar stenosis: angioplasty and follow-up
Abstract
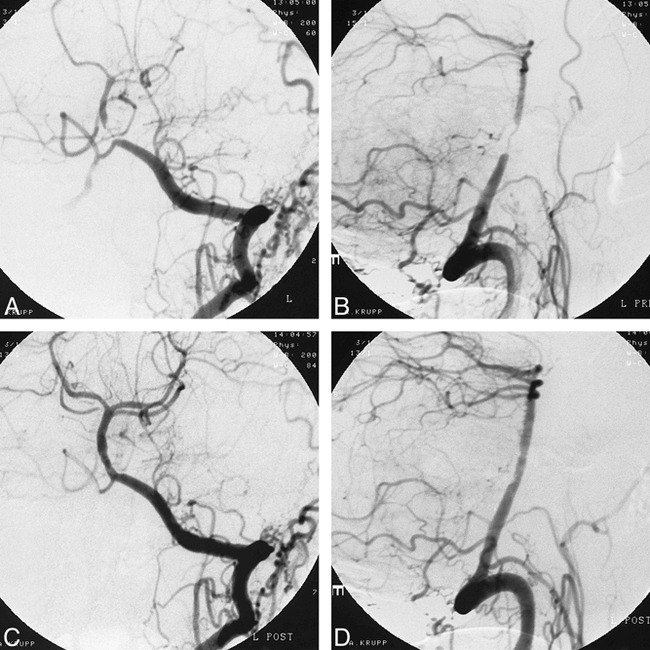
Background and purpose: When medication fails to improve symptoms of atherosclerotic stenosis of the intracranial vertebral and basilar arteries, percutaneous transluminal angioplasty (PTA) is considered. However, because investigators disagree on the usefulness of this procedure, we conducted a retrospective study to evaluate the indications, efficacy, and safety of PTA.
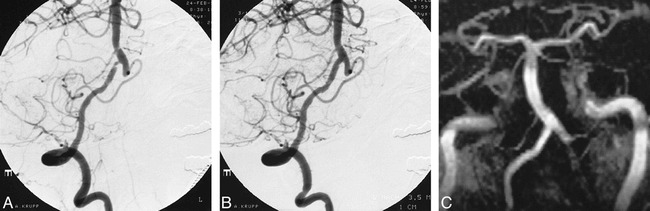
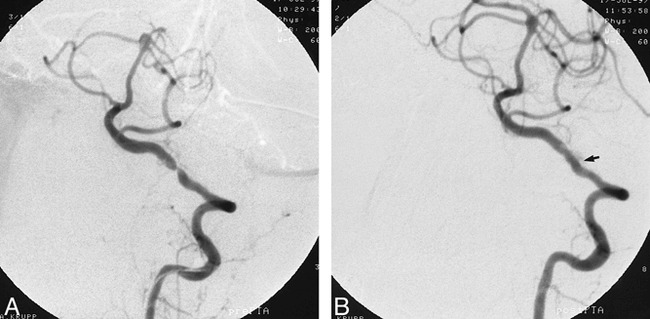
Methods: Twenty patients underwent PTA of the vertebral (n = 14) or basilar (n = 6) artery, 18 for neurologic signs and symptoms of arterial stenosis that recurred or progressed despite pharmacotherapy and two prophylactically. Neurologic examinations were performed before and after the procedure and arterial patency was evaluated at follow-up by digital subtraction angiography and/or MR angiography. Imaging follow-up was available for 14 (70%) of the 20 patients, neurologic follow-up for 15 (75%).
Results: The stenosis was successfully dilated in all patients, and on follow-up neuroradiologic examinations, vessel patency could be seen in 12 (86%) of 14 patients. Only one (7%) of 15 patients who returned for a follow-up neurologic examination had new symptoms (caused by occlusion of the vertebral artery 4 months after the procedure). One patient had a reversible neurologic deficit and one had hemiparesis after PTA. No patient died as a result of PTA.
Conclusion: In our study, PTA of intracranial vertebrobasilar arteries was associated with a low mortality and morbidity rate and with a high degree of patency. This technique may therefore be regarded as an effective means of improving the patency of stenotic arteries. In selective cases, it might be considered for use prophylactically.
Figures
References
-
- Stroke Prevention in Atrial Fibrillation Investigators. Adjusted-dose warfarin versus low-intensity, fixed dose warfarin plus aspirin for high-risk patients with atrial fibrillation: stroke prevention in atrial fibrillation III randomised clinical trial. Lancet 1996;348:633-638 - PubMed
-
- The Stroke Prevention in Reversible Ischemia Trial (SPIRIT) Study Group. A randomized trial of anticoagulants versus aspirin after cerebral ischemia of presumed arterial origin. Ann Neurol 1997;42:857-865 - PubMed
-
- Gorter JW, De Schryver EL, Algra A. Secondary prevention after ischemic cerebral infarct, the ESPRIT study: low dose anticoagulation, combined therapy with acetylsalicylic acid/dipyridamole or monotherapy with acetylsalicylic acid? Nervenarzt 1999;70:368-370 - PubMed
-
- Chimowitz MI, Kokkinos J, Strong J, et al. The warfarin-aspirin symptomatic intracranial disease study. Neurology 1995;45:1488-1493 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources