

Dynamic helical CT of T1 and T2 glottic carcinomas: predictive value for local control with radiation therapy
- PMID: 10954287
- PMCID: PMC8174922
Dynamic helical CT of T1 and T2 glottic carcinomas: predictive value for local control with radiation therapy
Abstract
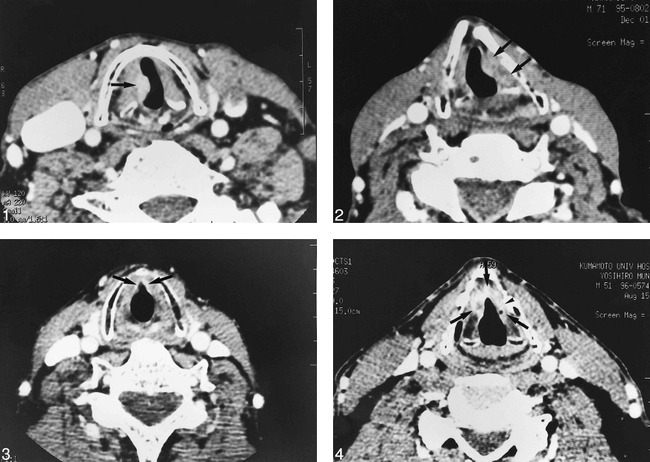
Background and purpose: Tumor volume and cartilage invasion have been suggested as prognostic factors of glottic carcinomas following definitive radiation therapy. Radiologic examinations provide additional information regarding the deep extension of tumor. We determined whether dynamic helical CT can predict local control of early (T1 and T2 stage) glottic carcinomas treated with definitive radiation therapy.
Methods: Sixty-eight patients with early glottic carcinoma evaluated on pretreatment dynamic helical CT were treated with definitive radiation therapy. Tumor detectability, maximum dimension, tumor volume, and involvement of anatomic subsites (anterior commissure, ventricle, subglottic region, and thyroid and arytenoid cartilages) were determined by consensus by three radiologists without previous knowledge of the clinical information. The CT findings were correlated with local control.
Results: The two-year local control rate was 76%; 91% for T1 and 60% for T2 lesions. Univariate analysis revealed clinical T stage, tumor detectability, maximum dimension, tumor volume, anterior commissure involvement, ventricle involvement, and thyroid cartilage involvement as significant prognostic factors. Thyroid cartilage involvement was an independent predictor by multivariate analysis. The lesions separate from the thyroid cartilage had a 95% probability of local control, whereas the lesions adjacent to the cartilage had only a 42% control rate.
Conclusion: Dynamic helical CT provides prognostic information for the results of definitive radiation therapy. Patients with a tumor adjacent to the thyroid cartilage had an increased risk of local failure.
Figures
References
-
- Mukherji SK, Pillsbury HR, Castillo M. Imaging squamous cell carcinoma of the upper aerodigestive tract: what clinicians need to know. Radiology 1997;205:629-646 - PubMed
-
- Million RR, Cassisi NJ, Mancuso AA. Larynx. In: Million RR, Cassisi NJ, eds. Management of Head and Neck Cancer: A Multidisciplinary Approach. 2nd ed. Philadelphia: Lippincott 1994 431-497
-
- Million RR. The larynx, so to speak: everything I wanted to know about laryngeal cancer I learned in the last 32 years. Int J Radiat Oncol Biol Phys 1992;23:691-704 - PubMed
-
- Le QT, Fu KK, Kroll S, et al. Influence of fraction size, total dose, and overall time on local control of T1-T2 glottic carcinoma. Int J Radiation Oncol Biol Phys 1997;39:115-126 - PubMed
-
- Fein DA, Mendenhall WM, Parsons JT, Million RR. T1-T2 squamous cell carcinoma of the glottic larynx treated with radiotherapy: a multivariate analysis of variables potentially influencing local control. Int J Radiat Oncol Biol Phys 1993;25:605-611 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical