

Case Reports
Intracranial and intraspinal meningeal melanocytosis
Affiliations
- PMID: 10954294
- PMCID: PMC8174895
Item in Clipboard
Case Reports
Intracranial and intraspinal meningeal melanocytosis
AJNR Am J Neuroradiol.
2000 Aug.
Abstract
We describe a 35-year-old man with a history of remote closed head injury who presented with new neurologic deficits. A noncontrast head CT scan showed hyperattenuation involving both temporal lobes, frontal lobes, basal meninges, and cerebellum. A subsequent contrast-enhanced MR examination of the brain showed enhancement in the basal cisterns extending into the upper cervical spine and throughout the spinal canal. Gross, histologic, and immunohistochemical analysis revealed meningeal melanocytoma.
Figures
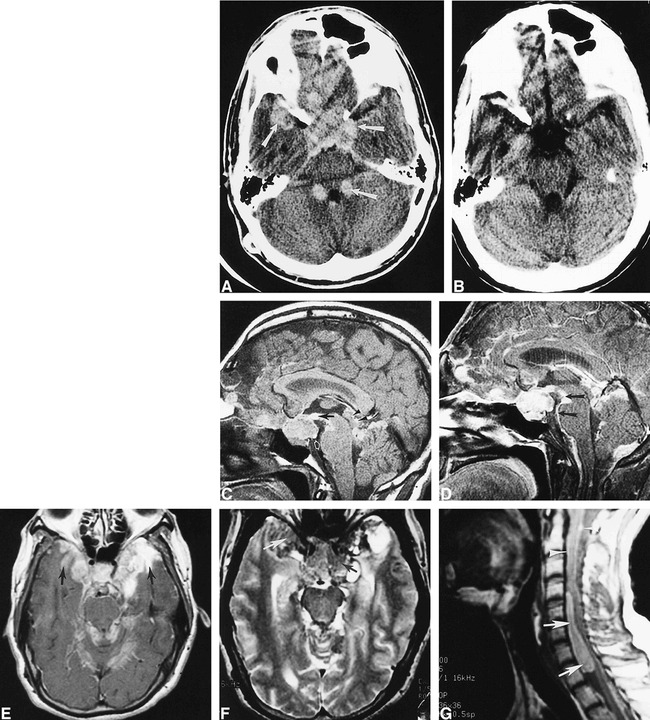
35-year-old man with a history of remote closed head injury who presented with recurrent headache, cortical blindness, and numerous new neurologic deficits. A, Axial noncontrast CT scan shows increased attenuation of the right temporal lobe, frontal lobes, suprasellar cistern, cerebellum, basal cisterns, dentate nuclei, and an area adjacent to the fourth ventricle (arrows). B, Axial noncontrast CT scan obtained 4 years earlier shows no areas of increased attenuation in the parasellar regions. C, Sagittal noncontrast T1-weighted MR image depicts a suprasellar mass along with areas of increased signal in the tuber cinereum (black arrow) and tectal region (arrowheads), consistent with T1 shortening from melanin. Note the subtle area of increased signal in the pons (white arrow). D, Contrast-enhanced MR image shows marked basal cistern involvement (arrows). E, Axial contrast-enhanced T1-weighted MR image of the brain shows enhancement of the basal meninges and intraparenchymal lesions of both temporal lobes (arrows). F, Corresponding axial FSE T2-weighted MR image shows heterogeneous signal intensity in the parasellar region with decreased signal intensity from areas of melanin (arrows). G, Sagittal noncontrast T1-weighted MR image reveals a large, hyperintense, oblong, anterior intraspinal mass (arrows). Note subtle areas of increased signal intensity surrounding the adjacent spinal cord anteriorly and posteriorly (arrowheads).
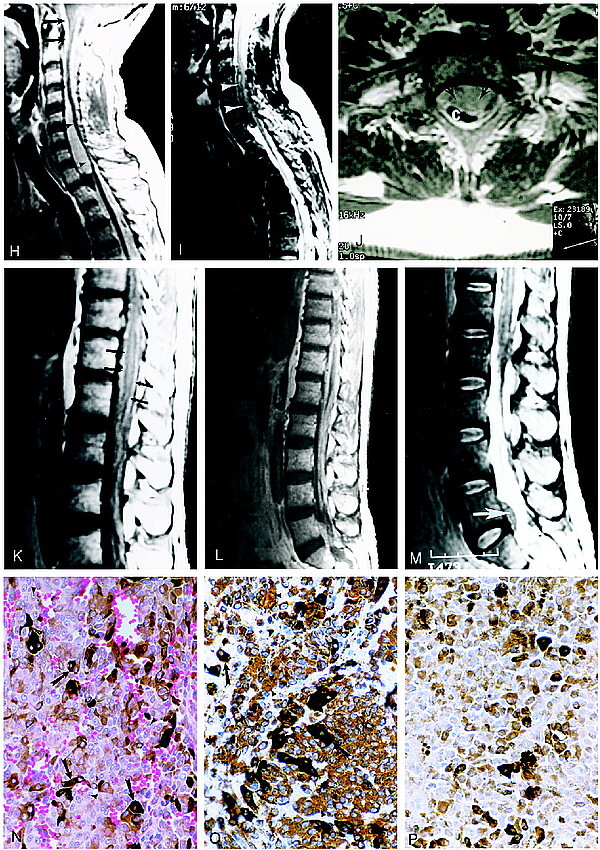
Continued. H, Sagittal contrast-enhanced T1-weighted MR image of the cervicothoracic spine shows extensive meningeal enhancement (arrows) with mass effect and spinal cord compression at the C4–T1 level (arrowheads). I, Sagittal FSE T2-weighted MR image reveals decreased signal intensity within the intraspinal mass caused by melanin deposits (arrowheads). J, Axial contrast-enhanced MR image shows marked compression of the cervical spinal cord by the mass (arrows). C indicates cervical spinal cord. K, Sagittal noncontrast T1-weighted MR image of the thoracic and lumbar spine shows increased signal intensity surrounding the conus medullaris (arrows). L, Sagittal contrast-enhanced T1-weighted MR image of the thoracolumbar spine shows extensive intradural enhancement and an anterior intraspinal mass at the L5–S1 level. M, Sagittal FSE T2-weighted MR image of the thoracic and lumbar spine shows decreased signal intensity in the intraspinal mass at the L5–S1 level (arrow). N, Photomicrograph of a mass in the left middle cranial fossa. The neoplasm contains sheets of cells, many of which contain dark brown melanin pigment (arrows). The nuclei are large and homogeneous with prominent nucleoli (arrowheads). Mitotic figures were rarely observed in the neoplasm (hematoxylin-eosin, original magnification ×560). O, Photomicrograph shows immunohistochemistry for vimentin. The tumor cells contain abundant intracytoplasmic staining for this intermediate filament, which is characteristic of melanocytoma (arrowheads). Other cells are darkly pigmented owing to melanin deposits (arrows). P, For comparison, this photomicrograph shows a control section containing only melanin deposits in which the primary antibody against vimentin was omitted. Immunohistochemical staining for HMB-45 and S-100 is not shown here (hematoxylin counterstain, original magnification ×560).
References
-
- Ruelle A, Tunesi G, Andrioli G. Spinal meningeal melanocytoma: case report and analysis of diagnostic criteria. Neurosurg Rev 1996;19:39-42 - PubMed
-
- Jellinger K, Bock H, Brenner H. Meningeal melanocytoma: report of a case and review of the literature. Acta Neurochir 1988;94:78-87 - PubMed
-
- Lach B, Russel N, Benoit B, Atack D. Cellular blue nevus (“melanocytoma”) of the spinal meninges: electron microscope and immunohistochemical features. Neurosurgery 1988;22:773-780 - PubMed
-
- Litofsky NS, Zee CS, Breeze RE, Chandrasoma PT. Meningeal melanocytoma: diagnostic criteria for a rare lesion. Neurosurgery 1992;31:945-947 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical