

Palliative chemotherapy for advanced colorectal cancer: systematic review and meta-analysis. Colorectal Cancer Collaborative Group
- PMID: 10968812
- PMCID: PMC27466
- DOI: 10.1136/bmj.321.7260.531
Palliative chemotherapy for advanced colorectal cancer: systematic review and meta-analysis. Colorectal Cancer Collaborative Group
Abstract
Objectives: To determine the benefits and harms of palliative chemotherapy in patients with locally advanced or metastatic colorectal cancer and to compare the outcomes for elderly and younger patients.
Design: Meta-analysis of individual patient data and published summary statistics from trials for which individual patient data could not be obtained from the investigators.
Studies: All randomised controlled trials comparing palliative chemotherapy with supportive care in patients with advanced colorectal cancer that were identified by computerised and hand searches of the literature, scanning references, and contacting investigators.
Main outcome measures: Survival, disease progression, quality of life, and toxicity.
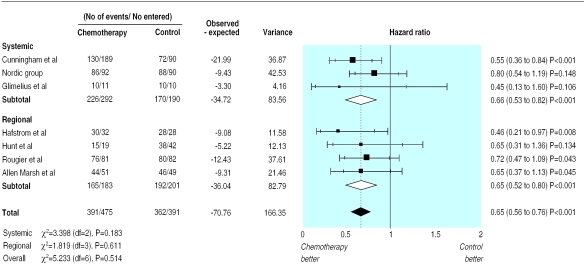
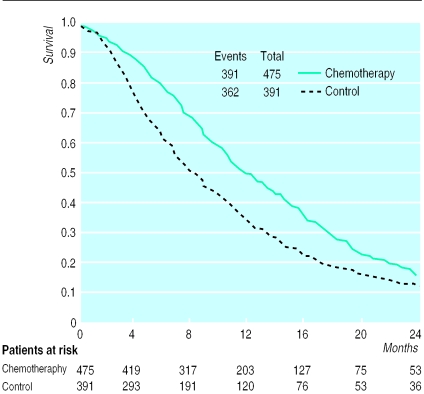
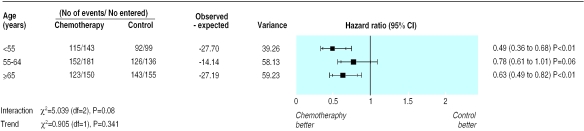
Results: 13 randomised controlled trials including a total of 1365 patients met the inclusion criteria. Meta-analysis of seven trials that provided individual patient data (866 patients) showed that palliative chemotherapy was associated with a 35% reduction in the risk of death (95% confidence interval 24% to 44%). This translates into an absolute improvement in survival of 16% at both six and 12 months and an improvement in median survival of 3.7 months. No age related differences were found in the effectiveness of chemotherapy, but elderly patients were under represented in trials. The overall quality of evidence relating to treatment toxicity, symptom control, and quality of life was poor.
Conclusions: Chemotherapy is effective in prolonging time to disease progression and survival in patients with advanced colorectal cancer. The survival benefit may be underestimated in this analysis as some patients in the control arms received chemotherapy.
Figures
Comment in
-
Chemotherapy for advanced colorectal cancer.BMJ. 2000 Sep 2;321(7260):521-2. doi: 10.1136/bmj.321.7260.521. BMJ. 2000. PMID: 10968797 Free PMC article. No abstract available.
-
Chemotherapy for advanced colorectal cancer. Patients need time to reflect on uncertainties surrounding palliative chemotherapy.BMJ. 2001 Jan 27;322(7280):234. BMJ. 2001. PMID: 11159629 No abstract available.
References
-
- Office for National Statistics. Cancer statistics registrations: England and Wales, 1992. London: Stationery Office; 1998.
-
- Office for National Statistics. Mortality statistics: cause, England and Wales 1997. London: Stationery Office; 1997.
-
- Cunningham D, Findlay M. The chemotherapy of colon cancer can no longer be ignored. Eur J Cancer. 1993;29A:2077–2079. - PubMed
-
- Seymour MT, Stenning SP, Cassidy J. Attitudes and practice in the management of metastatic colorectal cancer in Britain. Colorectal Cancer Working Party of the UK Medical Research Council. Clin Oncol. 1997;9:248–251. - PubMed
-
- Wils J, Sahmoud T, Sobrero A, Bleiberg H, Ahmedzai S, Blazeby J, et al. Evaluation of clinical efficacy of new medical treatments in advanced colorectal cancer. Results of a workshop organized by the EORTC GITCCG. Tumori. 1998;84:335–347. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous