

Comparative long-term evaluation of tacrolimus and cyclosporine in pediatric liver transplantation
- PMID: 10972220
- PMCID: PMC2962406
- DOI: 10.1097/00007890-200008270-00015
Comparative long-term evaluation of tacrolimus and cyclosporine in pediatric liver transplantation
Abstract
Background: In this report, we compare the long-term outcome of pediatric liver transplantation (LTx) patients maintained with tacrolimus-based and with cyclosporine (CsA)-based immunosuppressive therapy. We examine long-term patient and graft survival, the incidence of rejection, and immunosuppression-related complications.
Method: There were 233 consecutive primary LTx in children (ages <18 years) performed between October 1989 and December 1994 with tacrolimus-based immunosuppressive therapy (Group I). These were compared with 120 consecutive primary LTx performed with CsA-based immunosuppressive therapy between January 1988 and October 1989(Group II). Children in both groups were followed until July 1999. Mean follow-up was 91.41+/-17.7 months (range 55.6-117.8) for Group I, and 128+/-6.1 months (range 116.7-138.6) for Group II.
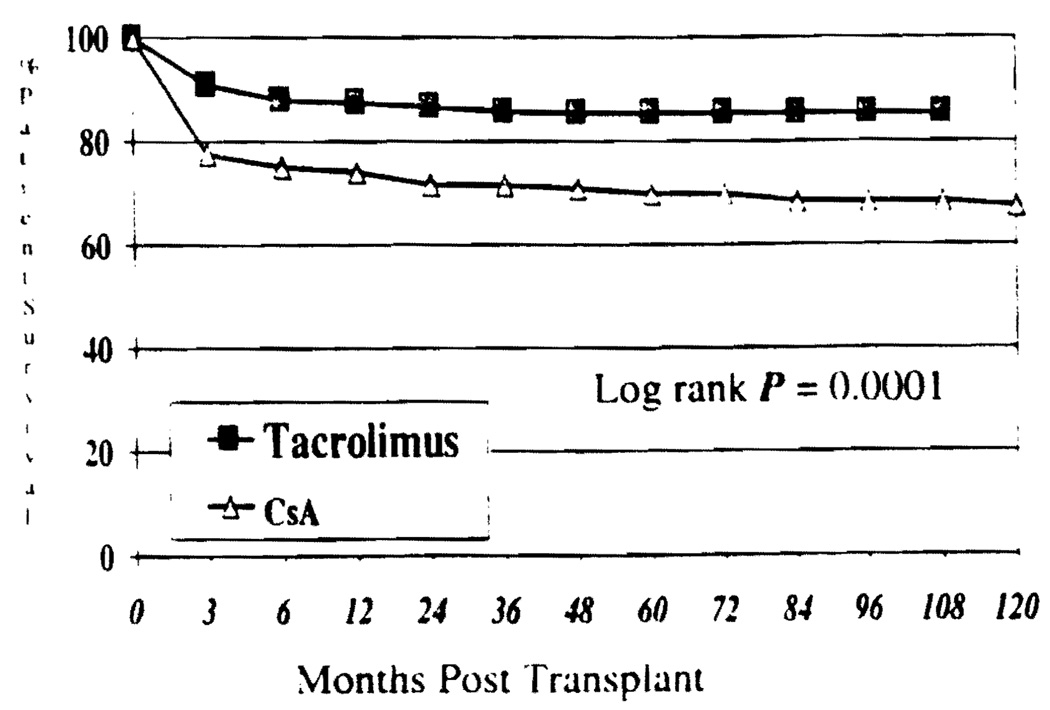
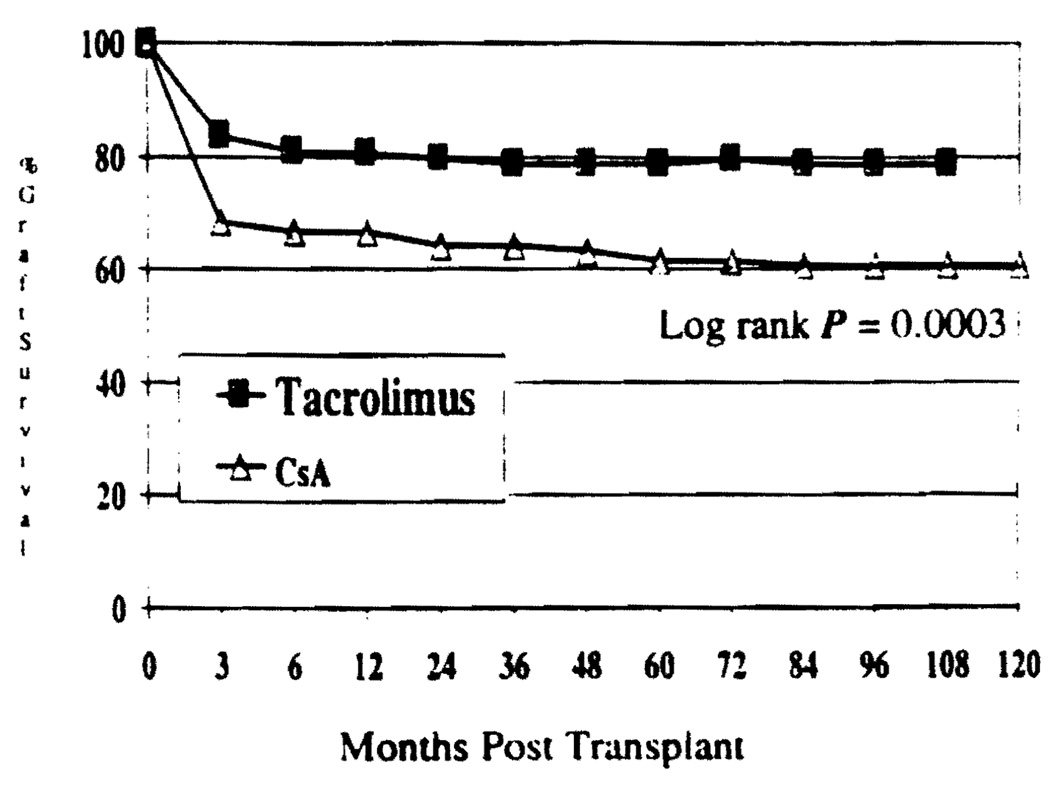
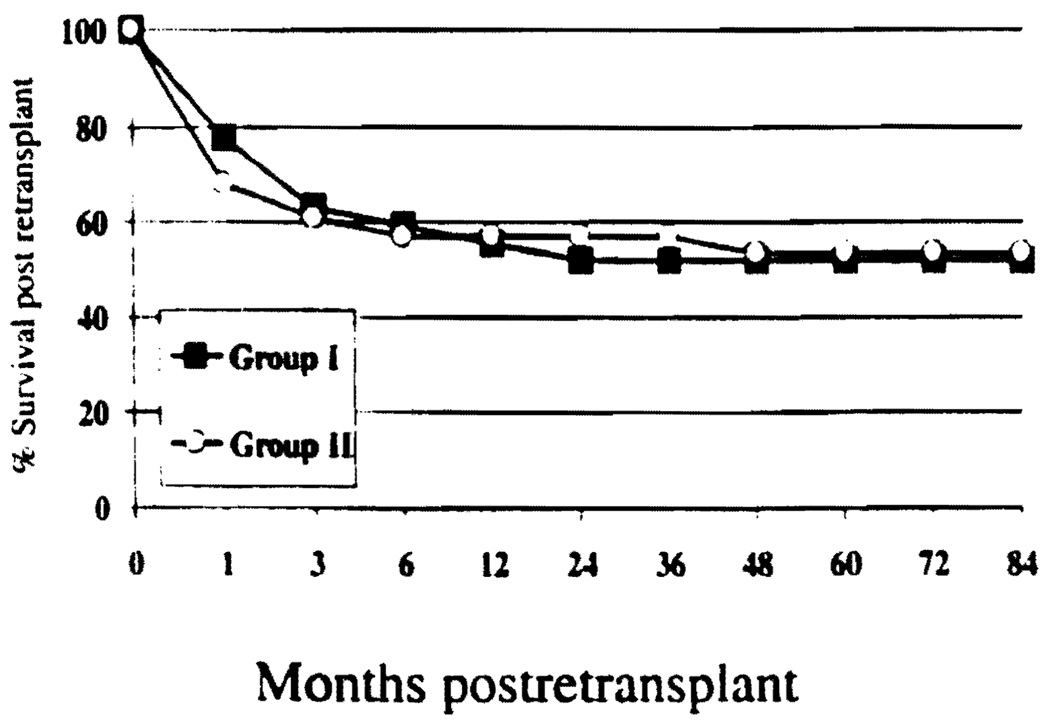
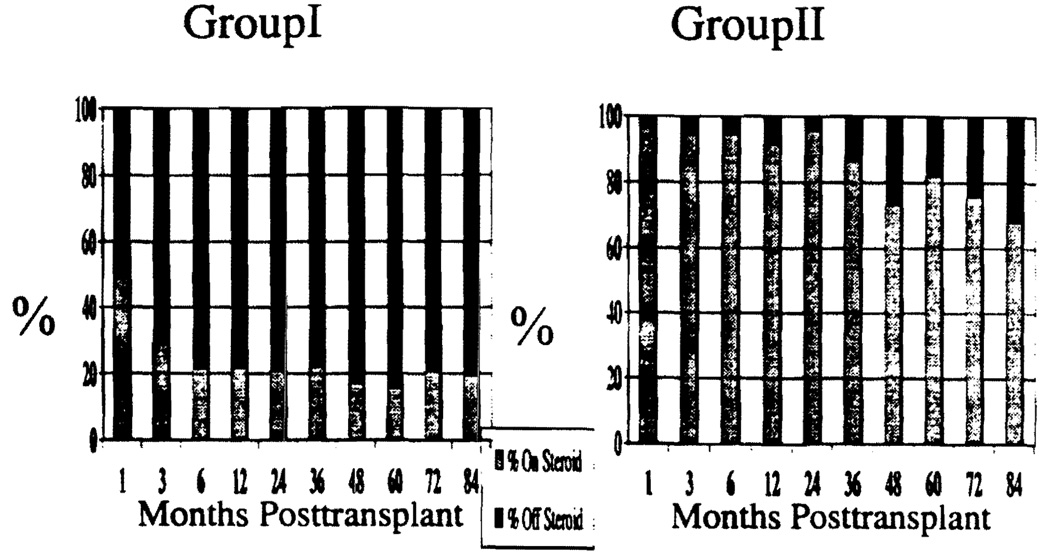
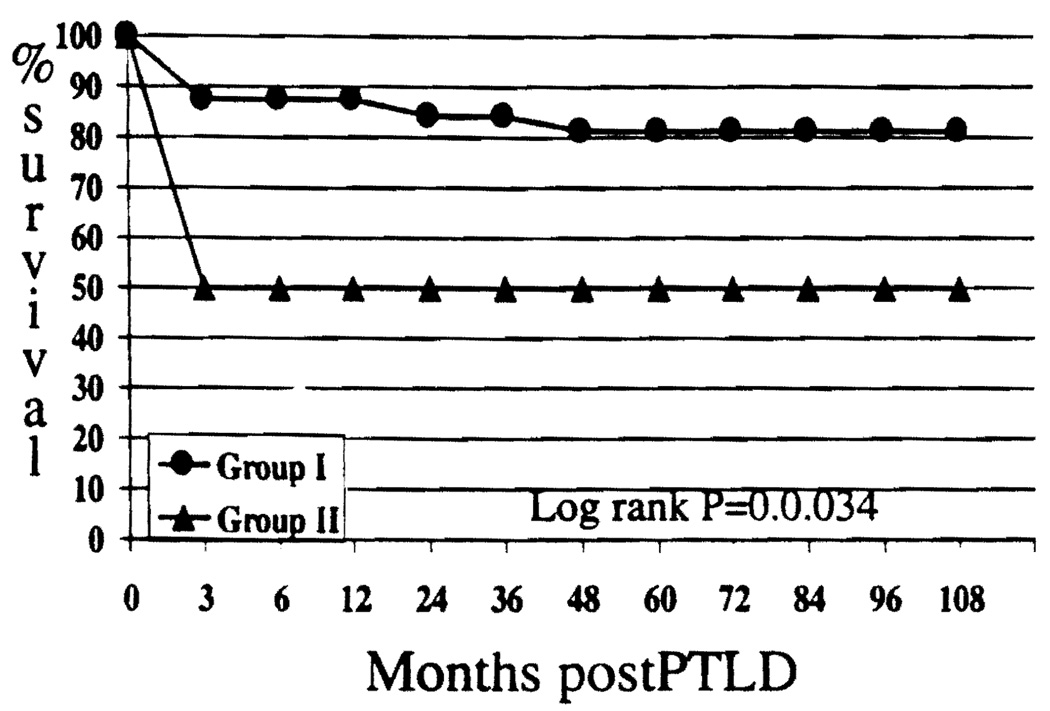
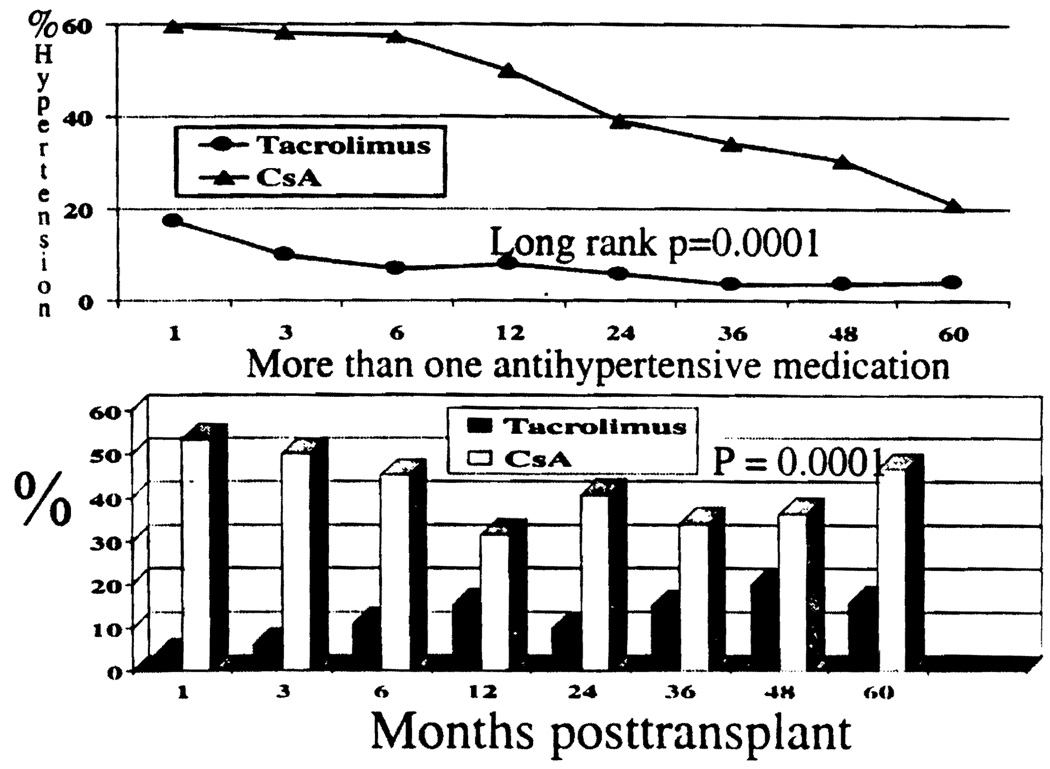
Results: At 9 years of follow-up, actuarial patient and graft survival were significantly improved (patient survival 85.41% in Group I vs. 63.8% in Group II, P=0.0001; graft survival Group I 78.9% vs. 60.8% Group II, P=0.0003) and the rate of re -transplantation was significantly lower among patients in Group I (12% in Group I vs. 22.5% in Group II P=0.01). Children in Group I also experienced a significantly reduced incidence of acute rejection (0.97 per patient Group I vs. 1.5 per patient Group II P=0.002) and significantly less steroid resistant acute rejection episodes (3.1% in Group I vs. 8.6% in Group II P=0.0001). The mean steroid dose was significantly lower in Group I compared with Group II at all time points (P=0.0001) after LTx. Freedom from steroid was also significantly higher in Group I compared with Group II at all time points after LTx (ranging from 78% to 84% in Group I and 9% to 32% in Group II during a 1- to 7-year posttransplant period P=0.0001). The rate of hypertension was significantly lower in Group I than Group II (P=0.0001), and the severity of hypertension (need for more than one anti-hypertensive medication) was also significantly lower in Group I than Group II (P=0.0001). Although the rate of posttransplant lymphoproliferative disorder (PTLD) was not significantly different (13.7% Group I vs.8.3% Group II, P=0.13), the survival after PTLD was significantly better for Group I at 81.2% than for Group II at 50% after 5 years (P=0.034). Conclusion. The results suggest that tacrolimus-based therapy provides significant long-term benefit to pediatric LTx patients, evidenced by significantly improved patient and graft survival, reduced rate of rejection, and hypertension with lower steroid doses.
Figures
References
-
- Reyes J, Mazariegos GV. Pediatric transplantation. Surg Clin North Am. 1999;79(1):163. - PubMed
-
- Alonso EM, Gonzalez-Vallina R, Whitington PF. Update of pediatric liver transplantation. Eur J Pediatr. 1992;151 suppl 1:S23. - PubMed
-
- Andrews W, Sommerauer J, Roden J, Andersen J, Conlin C, Moore P. 10 years of pediatric liver transplantation. J Pediatr Surg. 1996;31(5):619. - PubMed
-
- Andrews WS, Sommerauer J, Conlin C, Moore P. Comparison of cyclosporine- vs tacrolimus-based immunosuppression in pediatric liver transplantation. Transplant Proc. 1996;28(2):897. - PubMed
-
- Dhawan A, Muiesan P. Pediatric liver transplantation. Acta Paediatr Jpn. 1998;40(6):525. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
