

Predictors of survival after In vivo split liver transplantation: analysis of 110 consecutive patients
- PMID: 10973381
- PMCID: PMC1421145
- DOI: 10.1097/00000658-200009000-00003
Predictors of survival after In vivo split liver transplantation: analysis of 110 consecutive patients
Abstract
Objective: To determine the factors that influence patient survival after in vivo split liver transplantation (SLT).
Summary background data: Split liver transplantation is effective in expanding the donor pool, and its use reduces the number of deaths in patients awaiting orthotopic liver transplantation. Early SLTs were associated with poor outcomes, and acceptance of the technique has been slow. A better understanding of the factors that influence patient and graft survival would be useful in widening the application of SLT.
Methods: During a 3.5-year period, 55 right and 55 left lateral in vivo split grafts were transplanted in 102 pediatric and adult recipients. The authors' in vivo split technique has been previously described. Median follow-up was 14.5 months. Recipient, donor, and surgical variables were analyzed for their effect on patient survival after SLT.
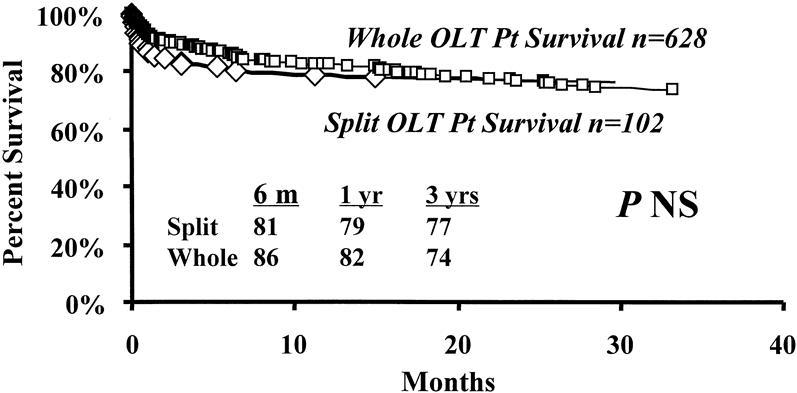
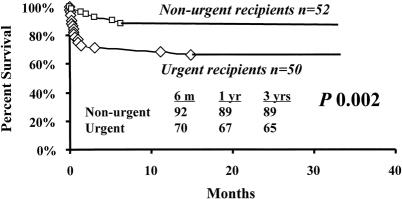
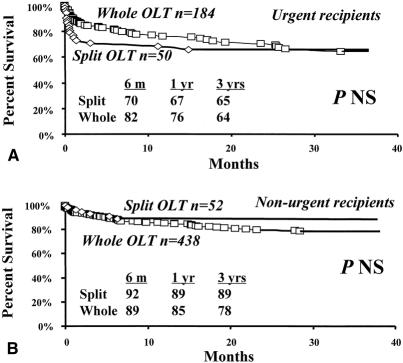
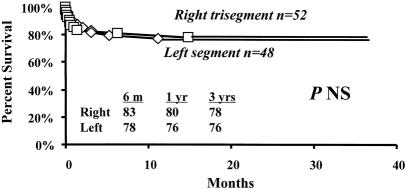
Results: Overall survival rates of patients who received an SLT were not significantly different from those of patients who received whole organ transplants. Survival of left lateral segment recipients, at median follow-up time, was 76% versus 80% in patients receiving a trisegment. Fifty of 102 patients (49%) were high-risk urgent recipients (United Network for Organ Sharing [UNOS] status 1 and 2A) and 52 (51%) were nonurgent recipients (UNOS status 2B, 3). High-risk recipients had a survival rate significantly lower than that of nonurgent recipients. By univariate comparison, two variables-UNOS status and number of transplants per patient-were significantly associated with an increased risk of death. Preoperative recipient mechanical ventilation, preoperative prothrombin time, donor sodium level, donor length of hospital stay, and warm ischemia time approached significance. The type of graft (right vs. left) did not reduce the survival rate after transplantation. Multivariate logistic regression analysis identified UNOS status and length of donor hospital stay as independent predictors of survival.
Conclusions: Patient survival of in vivo SLT is not significantly different from that of whole-organ orthotopic liver transplantation. The variables affecting outcome of in vivo SLT are similar to those in whole-organ transplantation. in vivo SLT should be widely applied to expand a severely depleted donor pool.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
