

Evolution in the management of hepatic trauma: a 25-year perspective
- PMID: 10973382
- PMCID: PMC1421146
- DOI: 10.1097/00000658-200009000-00004
Evolution in the management of hepatic trauma: a 25-year perspective
Abstract
Objective: To define the changes in demographics of liver injury during the past 25 years and to document the impact of treatment changes on death rates.
Summary background data: No study has presented a long-term review of a large series of hepatic injuries, documenting the effect of treatment changes on outcome. A 25-year review from a concurrently collected database of liver injuries documented changes in treatment and outcome.
Methods: A database of hepatic injuries from 1975 to 1999 was studied for changes in demographics, treatment patterns, and outcome. Factors potentially responsible for outcome differences were examined.
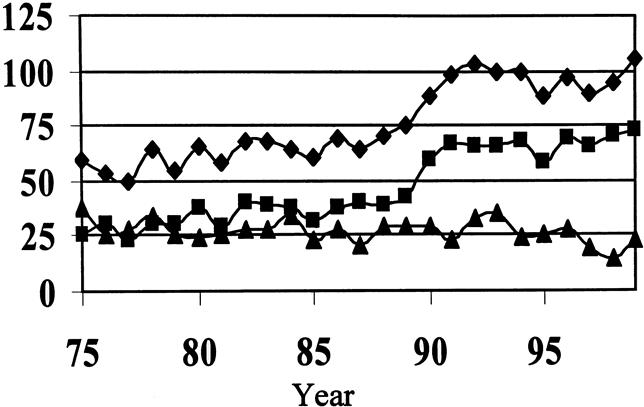
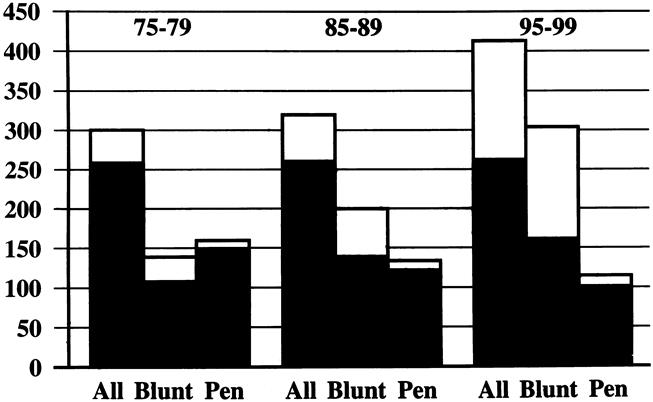
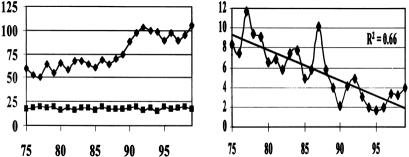
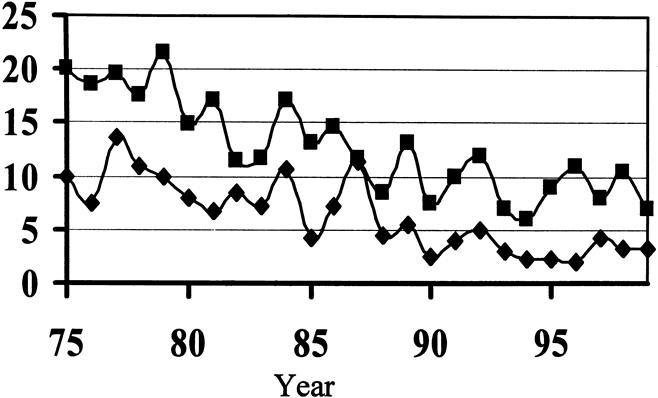
Results: A total of 1,842 liver injuries were treated. Blunt injuries have dramatically increased; the proportion of major injuries is approximately 16% annually. Nonsurgical therapy is now used in more than 80% of blunt injuries. The death rates from both blunt and penetrating trauma have improved significantly through each successive decade of the study. The improved death rates are due to decreased death from hemorrhage. Factors responsible include fewer major venous injuries requiring surgery, improved outcome with vein injuries, better results with packing, and effective arterial hemorrhage control with arteriographic embolization.
Conclusions: The treatment and outcome of liver injuries have changed dramatically in 25 years. Multiple modes of therapy are available for hemorrhage control, which has improved outcome.
Figures
References
-
- Moore EE, Shackford SR, Pachter HL, et al. Organ injury scaling: spleen, liver, kidney. J Trauma 1999; 29: 1664–1666. - PubMed
-
- Cue JI, Cryer HG, Miller FB, Richardson JD. Packing and planned re-exploration for hepatic and retroperitoneal hemorrhage: critical refinements of a useful technique. J Trauma 1990; 30: 1007–1013. - PubMed
-
- Feliciano DV, Mattox KL, Burch JM, et al. Packing for control of hepatic hemorrhage. J Trauma 1986; 26: 738–743. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
