

One hundred consecutive minimally invasive parathyroid explorations
- PMID: 10973383
- PMCID: PMC1421147
- DOI: 10.1097/00000658-200009000-00005
One hundred consecutive minimally invasive parathyroid explorations
Abstract
Objective: To review the outcomes of 100 consecutive minimally invasive parathyroid explorations.
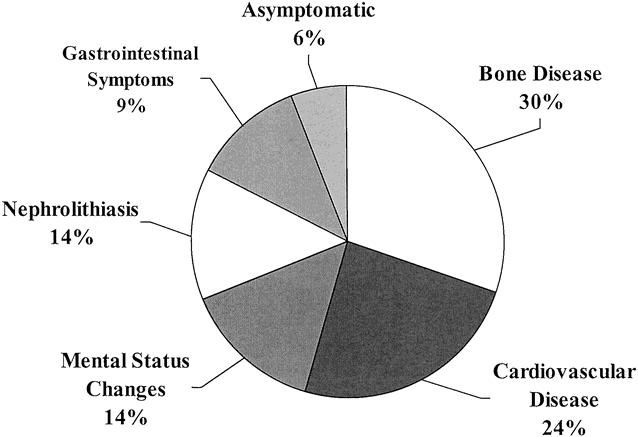
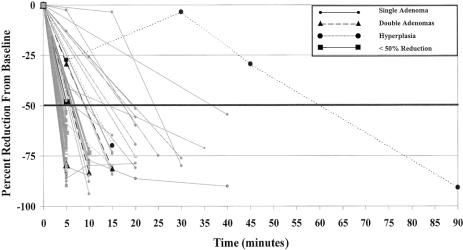
Summary background data: Minimally invasive parathyroidectomy (MIP) has challenged the traditional approach of bilateral neck exploration for patients with primary hyperparathyroidism. Most patients with primary hyperparathyroidism have a single adenoma that when resected results in cure. It therefore appears logical to perform a directed approach to adenoma extirpation. MIP involves high-quality sestamibi images obtained with single photon emission computed tomography to localize enlarged parathyroid glands in three dimensions, limited exploration after surgeon-administered cervical block anesthesia, rapid intraoperative parathyroid hormone assay to confirm the adequacy of resection, and discharge within 1 to 3 hours of surgery.
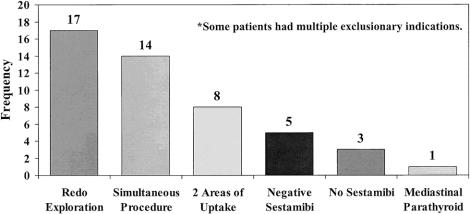
Methods: MIP was offered to 100 selected consecutive patients during an 18-month period beginning in March 1998.
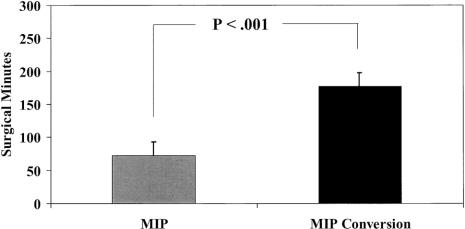
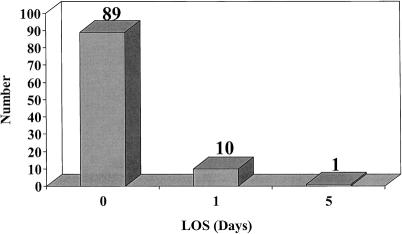
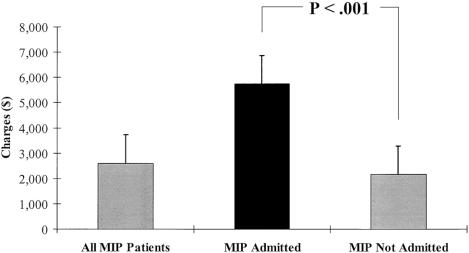
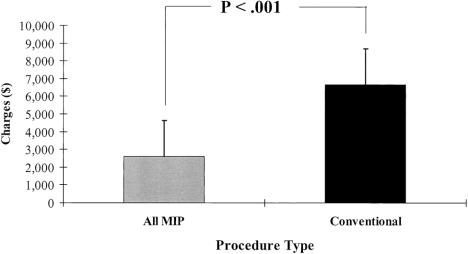
Results: Ninety-two cases were accomplished under cervical block anesthesia and 89 of these on an ambulatory basis. The cure rate was 100%, and there were no long-term complications. The mean hospital charge for MIP was less than 40% of that associated with traditional exploration.
Conclusions: Outpatient MIP appears to be the procedure of choice for most patients with primary hyperparathyroidism.
Figures
References
-
- Mandl F. Therapeutisher versuch bein einem falls von ostitis fibrosa generalisata mittles. Extirpation eines epithelkörperchen tumors. Wien Klin Wochenshr Zentral 1926; 143: 245–284.
-
- Carney JA. The glandulae parathyroideae of Ivar Sandström. Am J Surg Pathol 1996; 20: 1123–1144. - PubMed
-
- Chen H, Zeiger MA, Gordon TA, Udelsman R. Parathyroidectomy in Maryland: effects of an endocrine center. Surgery 1996; 120: 948–953. - PubMed
-
- Wang CA. Surgical management of primary hyperparathyroidism. Curr Probl Surg 1985; 22: 1–50. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
