

Radiofrequency ablation of hepatocellular cancer in 110 patients with cirrhosis
- PMID: 10973388
- PMCID: PMC1421151
- DOI: 10.1097/00000658-200009000-00010
Radiofrequency ablation of hepatocellular cancer in 110 patients with cirrhosis
Abstract
Objective: To determine the treatment efficacy, safety, local tumor control, and complications related to radiofrequency ablation (RFA) in patients with cirrhosis and unresectable hepatocellular carcinoma (HCC).
Summary background data: Most patients with HCC are not candidates for resection because of tumor size, location, or hepatic dysfunction related to cirrhosis. RFA is a technique that permits in situ destruction of tumors by means of local tissue heating.
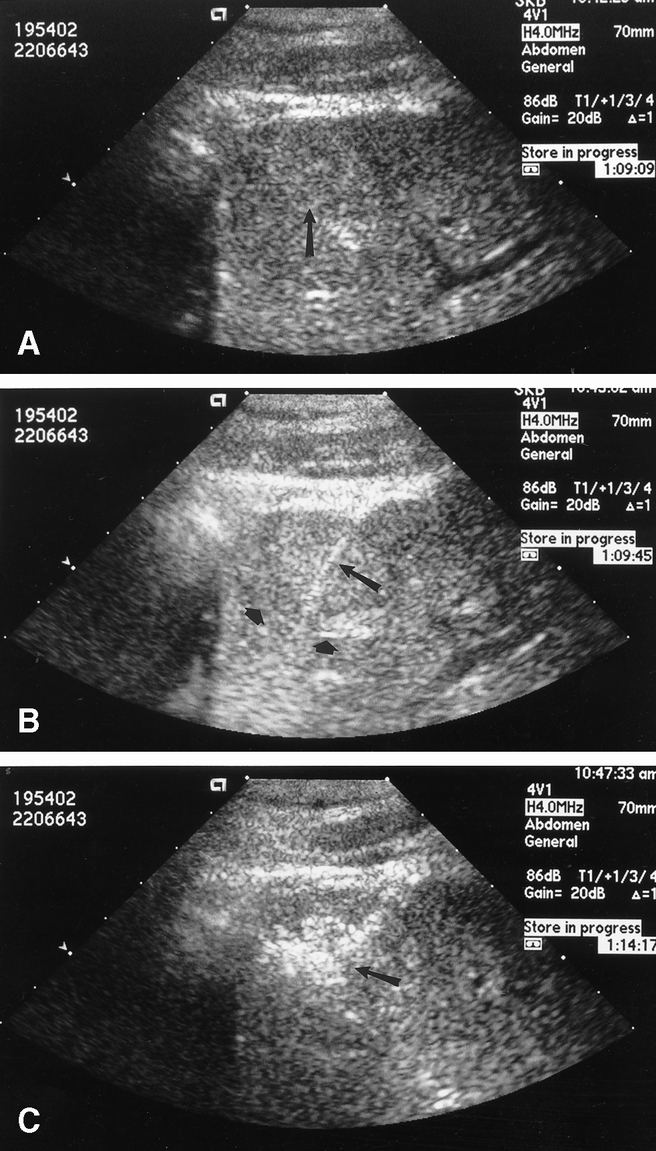
Methods: One hundred ten patients with cirrhosis and HCC (Child class A, 50; B, 31; C, 29) were treated during a prospective study using RFA. Patients were treated with RFA using an open laparotomy, laparoscopic, or percutaneous approach with ultrasound guidance to place the RF needle electrode into the hepatic tumors. All patients were followed up at regular intervals to detect treatment-related complications or recurrence of disease.
Results: All 110 patients were followed up for at least 12 months after RFA (median follow-up 19 months). Percutaneous or intraoperative RFA was performed in 76 (69%) and 34 patients (31%), respectively. A total of 149 discrete HCC tumor nodules were treated with RFA. The median diameter of tumors treated percutaneously (2.8 cm) was smaller than that of lesions treated during laparotomy (4.6 cm). Local tumor recurrence at the RFA site developed in four patients (3.6%); recurrent HCC subsequently developed in other areas of the liver in all four. New liver tumors or extrahepatic metastases developed in 50 patients (45. 5%), but 56 patients (50.9%) had no evidence of recurrence. There were no treatment-related deaths, but complications developed in 14 patients (12.7%) after RFA.
Conclusions: In patients with cirrhosis and HCC, RFA produces effective local control of disease in a significant proportion of patients and can be performed safely with minimal complications.
Figures
References
-
- Watkins KT, Curley SA. Liver and bile ducts. In: Abeloff MD, Armitage JO, Lichter AS, Niederhuber JE, eds. Clinical Oncology, 2nd ed. New York: Churchill Livingstone; 2000: 1681–1748.
-
- Williams I. Epidemiology of hepatitis C in the United States. Am J Med 1999; 107: 2S–9S. - PubMed
-
- Guadagnino V, Stroffolini T, Rapicetta M, et al. Prevalence, risk factors, and genotype distribution of hepatitis C virus infection in the general population: a community-based survey in southern Italy. Hepatology 1997; 26: 1006–1011. - PubMed
-
- Fan S-T, Ng IOL, Poon RTP, et al. Hepatectomy for hepatocellular carcinoma. The surgeon’s role in long-term survival. Arch Surg 1999; 134: 1124–1130. - PubMed
-
- Nagasue N. Liver resection for hepatocellular carcinoma: indications, techniques, complications, and prognostic factors. J Hepatobil Pancr Surg 1998; 5: 7–13. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
