

Postoperative bile duct strictures: management and outcome in the 1990s
- PMID: 10973393
- PMCID: PMC1421156
- DOI: 10.1097/00000658-200009000-00015
Postoperative bile duct strictures: management and outcome in the 1990s
Abstract
Objective: To describe the management and outcome after surgical reconstruction of 156 patients with postoperative bile duct strictures managed in the 1990s.
Summary background data: The management of postoperative bile duct strictures and major bile duct injuries remains a challenge for even the most skilled biliary tract surgeon. The 1990s saw a dramatic increase in the incidence of bile duct strictures and injuries from the introduction and widespread use of laparoscopic cholecystectomy. Although the management of these injuries and short-term outcome have been reported, long-term follow-up is limited.
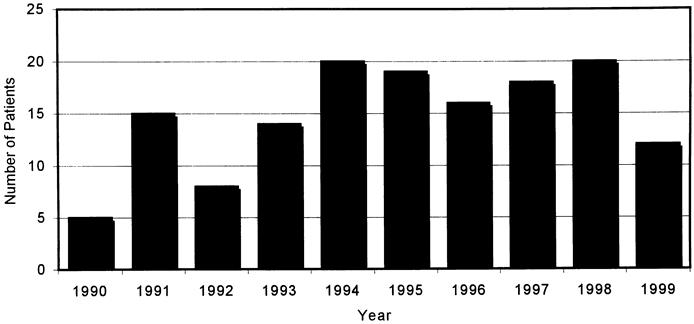
Methods: Data were collected prospectively on 156 patients treated at the Johns Hopkins Hospital with major bile duct injuries or postoperative bile duct strictures between January 1990 and December 1999. With the exception of bile duct injuries discovered and repaired during surgery, all patients underwent preoperative percutaneous transhepatic cholangiography and placement of transhepatic biliary catheters before surgical repair. Follow-up was conducted by medical record review or telephone interview during January 2000.
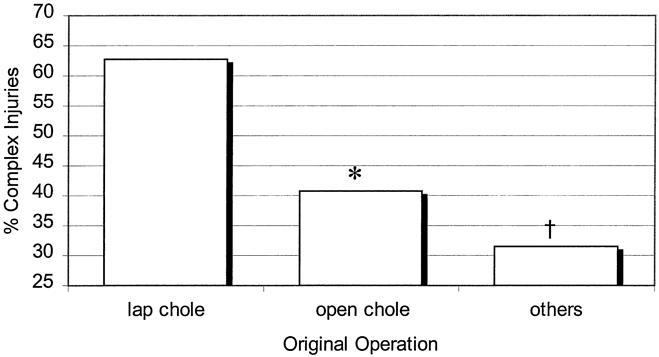
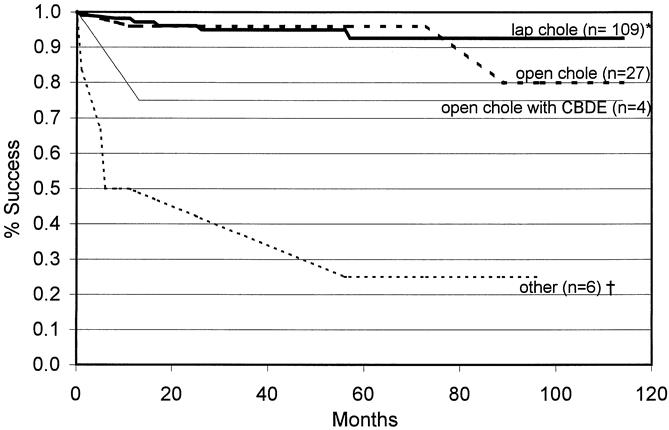
Results: Of the 156 patients undergoing surgical reconstruction, 142 had completed treatment with a mean follow-up of 57.5 months. Two patients died of reasons unrelated to biliary tract disease before the completion of treatment. Twelve patients (7.9%) had not completed treatment and still had biliary stents in place at the time of this report. Of patients who had completed treatment, 90. 8% were considered to have a successful outcome without the need for follow-up invasive, diagnos tic, or therapeutic interventional procedures. Patients with reconstruction after injury or stricture after laparoscopic cholecystectomy had a better overall outcome than patients whose postoperative stricture developed after other types of surgery. Presenting symptoms, number of stents, interval to referral, prior repair, and length of postoperative stenting were not significant predictors of outcome. Overall, a successful outcome, without the need for biliary stents, was obtained in 98% of patients, including those requiring a secondary procedure for recurrent stricture.
Conclusions: Major bile duct injuries and postoperative bile duct strictures remain a considerable surgical challenge. Management with preoperative cholangiography to delineate the anatomy and placement of percutaneous biliary catheters, followed by surgical reconstruction with a Roux-en-Y hepaticojejunostomy, is associated with a successful outcome in up to 98% of patients.
Figures
References
-
- Deziel DJ, Millikan KW, Economou SG, et al. Complications of laparoscopic cholecystectomy: a national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg 1993; 165: 9–14. - PubMed
-
- Orlando R III, Russell JC, Lynch J, Mattie A. Laparoscopic cholecystectomy: a statewide experience. Arch Surg 1993; 128: 494–499. - PubMed
-
- Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg 1995; 180: 101–125. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
