

Laparoscopic repair of gastric volvulus
- PMID: 10987399
- PMCID: PMC3113174
Laparoscopic repair of gastric volvulus
Abstract
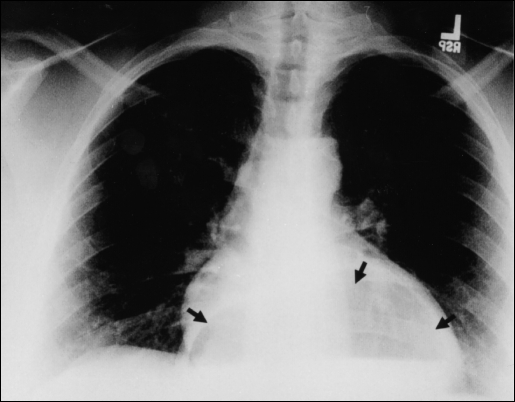
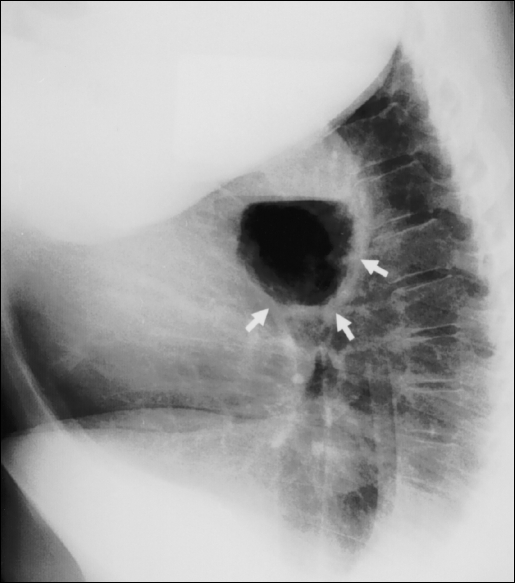
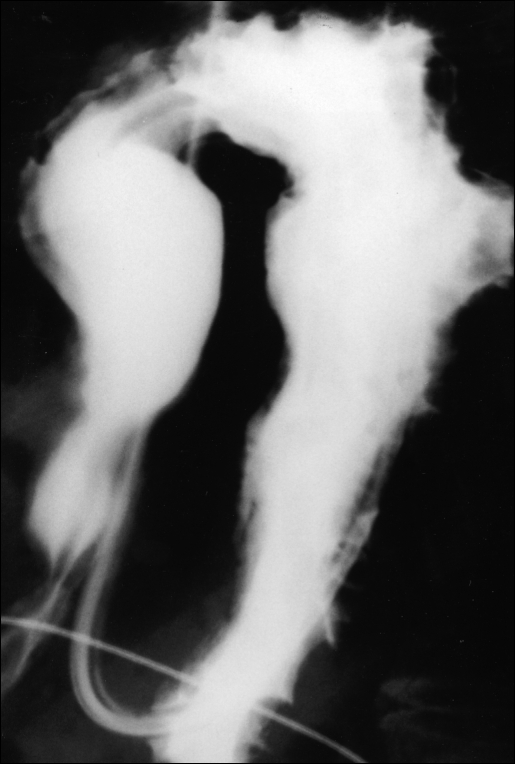
Background and objectives: Acute and chronic gastric volvulus usually present with different symptoms and affect patients primarily after the fourth decade of life. Volvulus can be diagnosed by an upper gastrointestinal contrast study or by esophagogastroduodenoscopy. There are three types of gastric volvulus: 1) organoaxial (most common type); 2) mesenteroaxial; and 3) a combination of the two. If undetected or if a delay in diagnosis and treatment occurs, serious complications can develop.
Methods: We present four cases of surgical repair of organoaxial volvulus consisting of laparoscopic reduction of the volvulus with excision of the hernia sac and reapproximation of the diaphragmatic crura. A Nissen fundoplication, to prevent reflux, was performed, and the stomach was pexed to the anterior abdominal wall by laparoscopic placement of a gastrostomy tube, thus preventing recurrent volvulus.
Results: There were no operative complications, and all four patients tolerated the procedure well. The patients were discharged one to three days postoperatively and were asymptomatic within two months.
Conclusion: With the advancement of laparoscopic Nissen fundoplication and laparoscopic repair of paraesophageal and hiatal hernias, minimally invasive surgical repair is possible. Based on our experience, we advocate the laparoscopic technique to repair gastric volvulus.
Figures


References
-
- Borchardt M. Zun pathologie and therapy des magnevolvulus. Arch Klin Chir. 1904;74:243–248
-
- Carter R, Rewer LA, Hinshaw DB. Acute gastric volvulus. Am J Surg. 1980;140:99–106 - PubMed
-
- Dalgaard JB. Volvulus of the stomach. Acta Clin Scand. 1952;103:131 - PubMed
-
- Llaneza PP, Salt WB. Gastric volvulus more common than previously thought. Postgrad Med. 1986;80:279–288 - PubMed
-
- Tanner CA. Chronic and recurrent volvulus of the stomach. Am J Surg. 1968;115:505–515 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources