

CC chemokine receptor 2 is critical for induction of experimental autoimmune encephalomyelitis
- PMID: 10993920
- PMCID: PMC2193286
- DOI: 10.1084/jem.192.6.899
CC chemokine receptor 2 is critical for induction of experimental autoimmune encephalomyelitis
Abstract
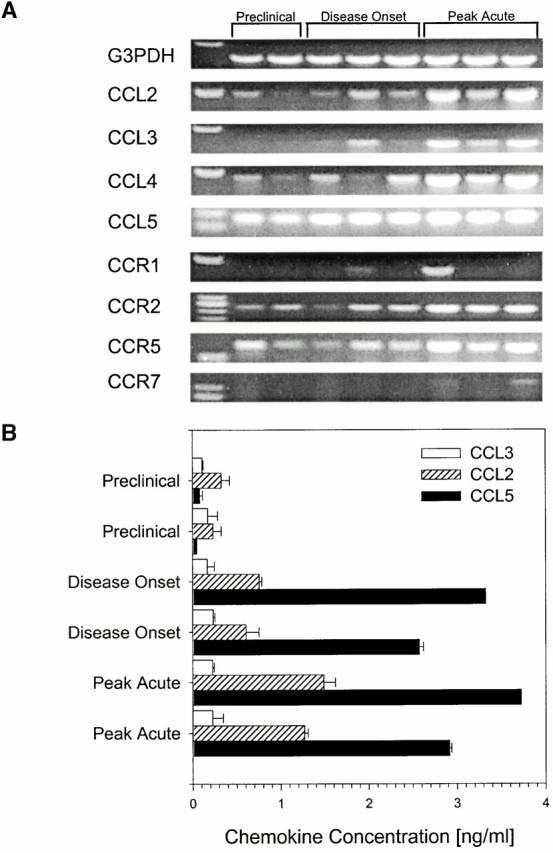
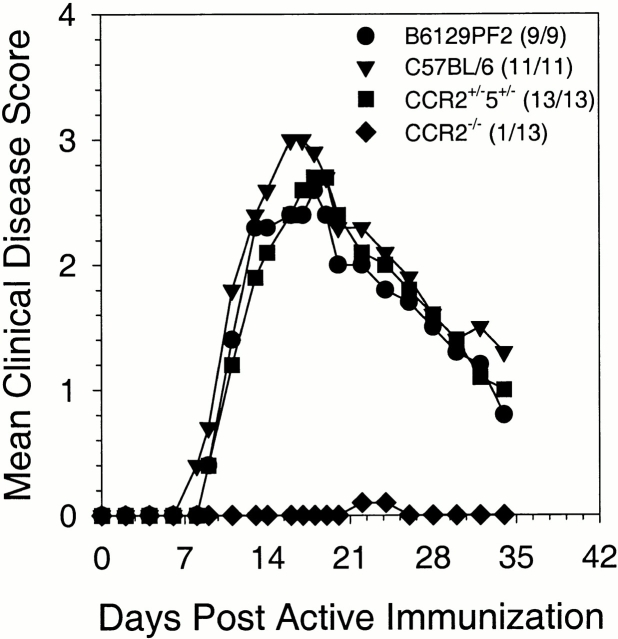
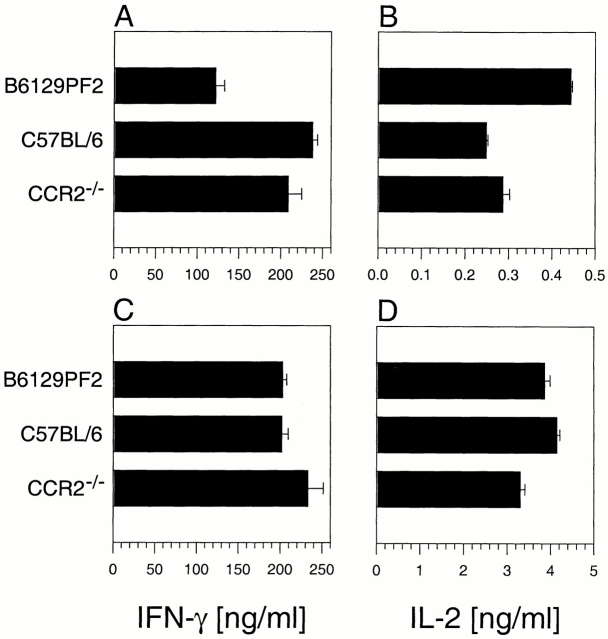
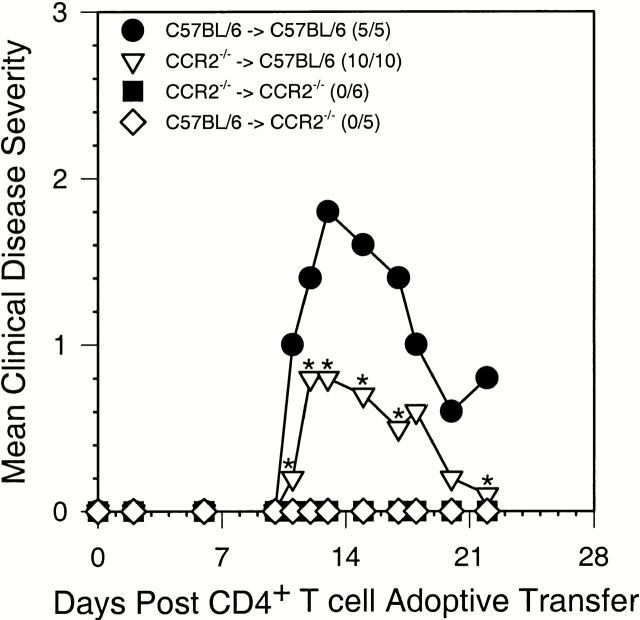
Experimental autoimmune encephalomyelitis (EAE) is a CD4(+) T lymphocyte-mediated disease of the central nervous system (CNS) characterized by mononuclear cell infiltration, demyelination, and paralysis. We previously demonstrated a role for chemokines in acute and relapsing EAE pathogenesis. Presently, we investigated the role of CC chemokine receptor 2 (CCR2) in acute EAE. CCR2(-/-) mice did not develop clinical EAE or CNS histopathology, and showed a significant reduction in T cell- and CNS-infiltrating CD45(high)F4/80(+) monocyte subpopulations. Peripheral lymphocytes from CCR2(-/-) mice produced comparable levels of interferon-gamma (IFN-gamma) and interleukin (IL)-2 in response to antigen-specific restimulation when compared with control mice. Adoptively transferred myelin oligodendrocyte glycoprotein 35-55-specific T cells lacking expression of CCR2 were able to induce EAE, whereas CCR2(-/-) recipients of wild-type T cells failed to develop disease. These results suggest that CCR2 expression on host-derived mononuclear cells is critical for disease induction.
Figures
References
-
- Hohlfeld R. Biotechnological agents for the immunotherapy of multiple sclerosis. Principles, problems, and perspectives. Brain. 1997;120:865–916. - PubMed
-
- Krakowski M.L., Owens T. The central nervous system environment controls effector CD4+ T cell cytokine profile in experimental allergic encephalomyelitis. Eur. J. Immunol. 1997;27:2840–2847. - PubMed
-
- Hickey W.F., Hsu B.L., Kimura H. T-lymphocyte entry into the central nervous system. J. Neurosci. Res. 1991;28:254–260. - PubMed
-
- Cross A.H., Cannella B., Brosnan C.F., Raine C.S. Homing to central nervous system vasculature by antigen-specific lymphocytes. I. Localization of 14C-labeled cells during acute, chronic, and relapsing experimental allergic encephalomyelitis. Lab. Invest. 1990;63:162–170. - PubMed
-
- Yednock T.A., Cannon C., Fritz L.C., Sanchez-Madrid F., Steinman L., Karin N. Prevention of experimental autoimmune encephalomyelitis by antibodies against α4β1 integrin. Nature. 1992;356:63–66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
