

Functional human T-cell immunity and osteoprotegerin ligand control alveolar bone destruction in periodontal infection
- PMID: 10995794
- PMCID: PMC3102542
- DOI: 10.1172/jci10763
Functional human T-cell immunity and osteoprotegerin ligand control alveolar bone destruction in periodontal infection
Abstract
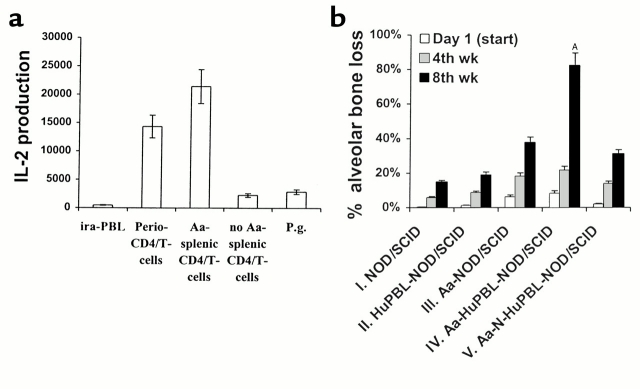
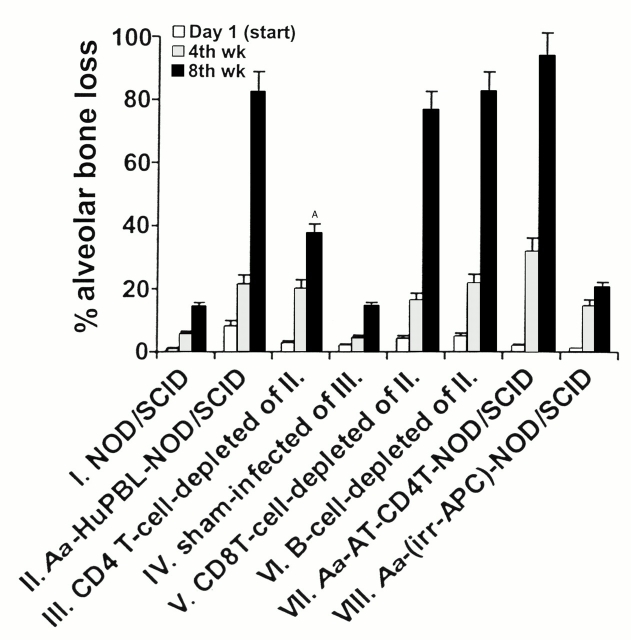
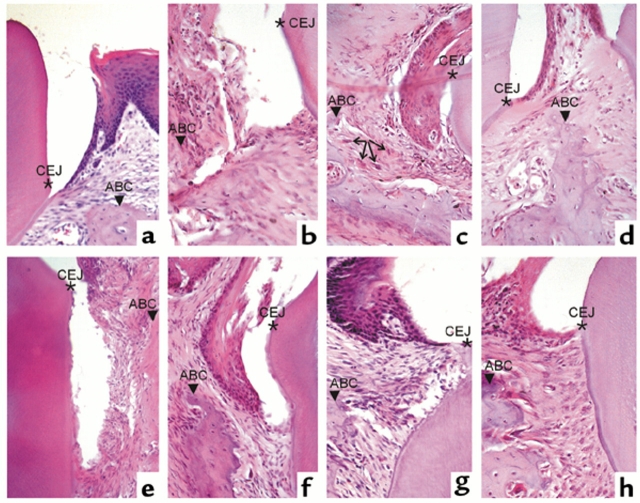
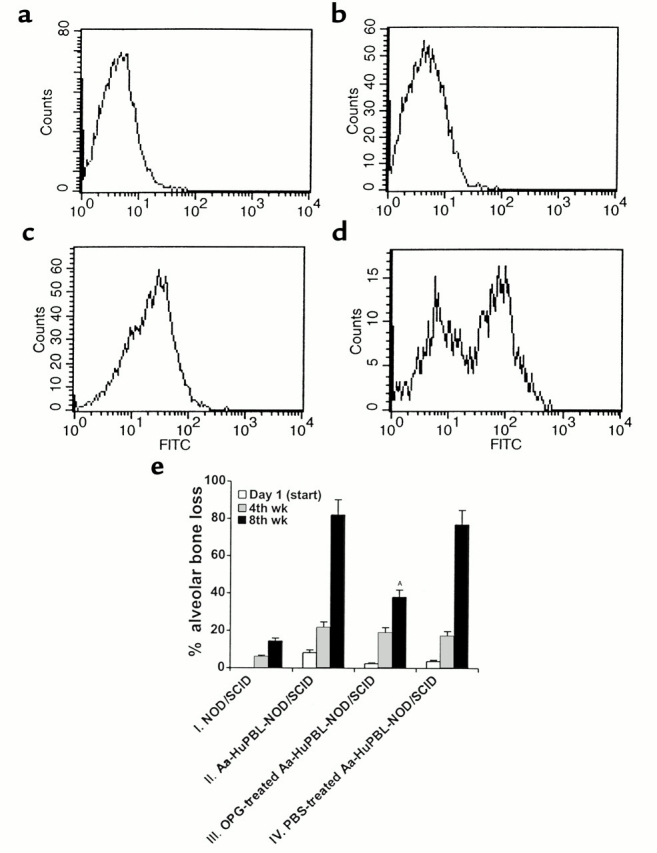
Periodontitis, a prime cause of tooth loss in humans, is implicated in the increased risk of systemic diseases such as heart failure, stroke, and bacterial pneumonia. The mechanisms by which periodontitis and antibacterial immunity lead to alveolar bone and tooth loss are poorly understood. To study the human immune response to specific periodontal infections, we transplanted human peripheral blood lymphocytes (HuPBLs) from periodontitis patients into NOD/SCID mice. Oral challenge of HuPBL-NOD/SCID mice with Actinobacillus actinomycetemcomitans, a well-known Gram-negative anaerobic microorganism that causes human periodontitis, activates human CD4(+) T cells in the periodontium and triggers local alveolar bone destruction. Human CD4(+) T cells, but not CD8(+) T cells or B cells, are identified as essential mediators of alveolar bone destruction. Stimulation of CD4(+) T cells by A. actinomycetemcomitans induces production of osteoprotegerin ligand (OPG-L), a key modulator of osteoclastogenesis and osteoclast activation. In vivo inhibition of OPG-L function with the decoy receptor OPG diminishes alveolar bone destruction and reduces the number of periodontal osteoclasts after microbial challenge. These data imply that the molecular explanation for alveolar bone destruction observed in periodontal infections is mediated by microorganism-triggered induction of OPG-L expression on CD4(+) T cells and the consequent activation of osteoclasts. Inhibition of OPG-L may thus have therapeutic value to prevent alveolar bone and/or tooth loss in human periodontitis.
Figures
Comment in
-
Interactions between immune and bone cells: new insights with many remaining questions.J Clin Invest. 2000 Sep;106(6):749-52. doi: 10.1172/JCI11089. J Clin Invest. 2000. PMID: 10995785 Free PMC article. No abstract available.
References
-
- Clark WB, Loe H. Mechanisms of initiation and progression of periodontal disease. Periodontol 2000. 1993;2:72–82. - PubMed
-
- Brown LJ, Oliver RC, Loe H. Evaluating periodontal status of US employed adults. J Am Dent Assoc. 1990;121:226–232. - PubMed
-
- Eklund SA, Burt BA. Risk factors for total tooth loss in the United States; longitudinal analysis of national data. J Public Health Dent. 1994;54:5–14. - PubMed
-
- Genco R. Research news. Healthy gums for a happy heart. Science. 1997;276:203.
-
- Mattila KL, Valle MS, Nieminen MS, Valtonen VV, Hietaniemi KL. Dental infections and coronary atherosclerosis. Atherosclerosis. 1993;103:205–211. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
