

Gallbladder cancer: comparison of patients presenting initially for definitive operation with those presenting after prior noncurative intervention
- PMID: 10998654
- PMCID: PMC1421188
- DOI: 10.1097/00000658-200010000-00011
Gallbladder cancer: comparison of patients presenting initially for definitive operation with those presenting after prior noncurative intervention
Abstract
Objective: To compare patients with gallbladder cancer presenting for therapy with and without prior operation elsewhere to determine if an initial noncurative procedure alters outcome.
Summary background data: Nihilism has traditionally surrounded treatment of gallbladder cancer, particularly since the majority of cases are discovered during exploration for presumed gallstone disease when unsuspected cancers cannot be handled definitively and tumor is often violated.
Methods: Presentation, operative data, complications, and survival were examined for 410 patients presenting between July 1986 and March 2000. In particular, the 248 patients presenting for therapy after prior operation elsewhere were compared with the remainder who presented without prior operation to determine if an initial noncurative procedure alters outcome.
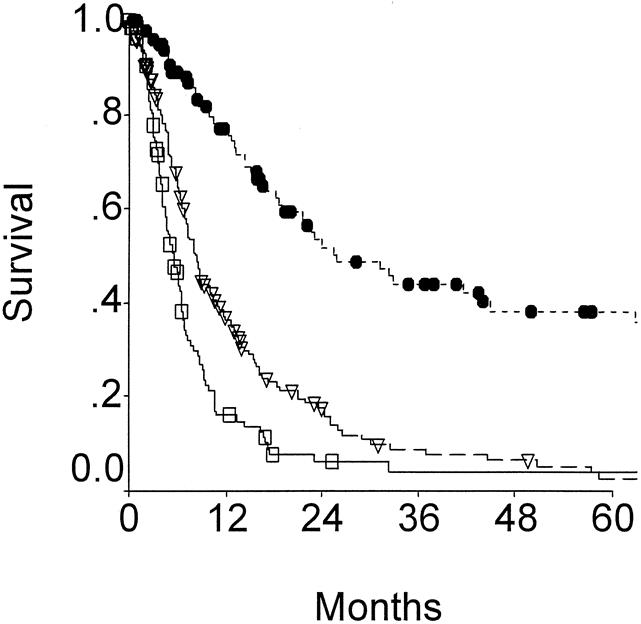
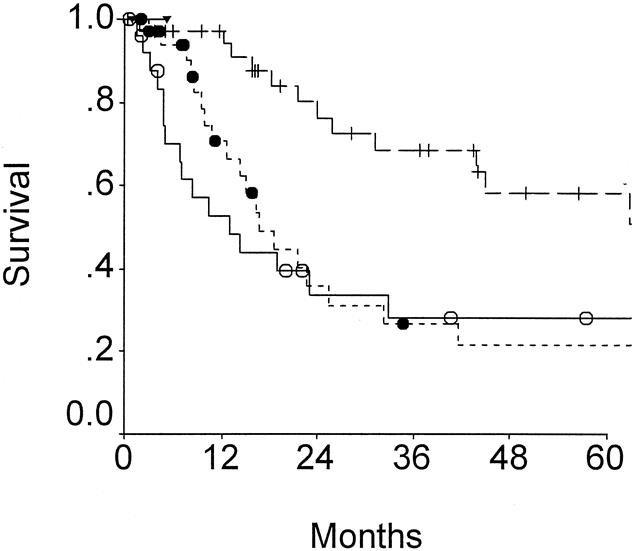
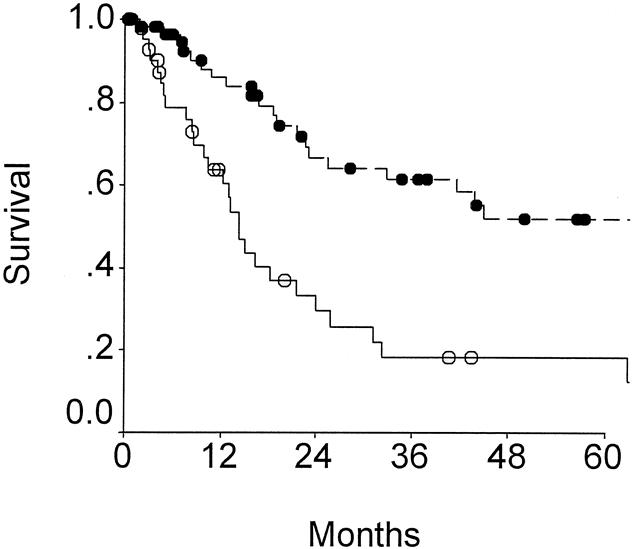
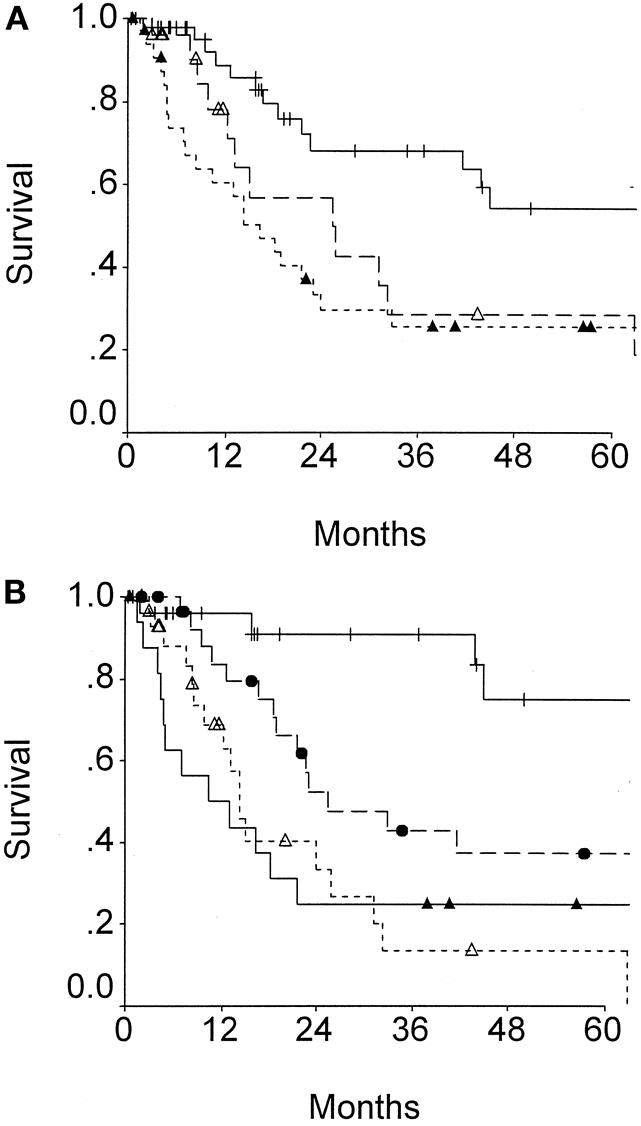
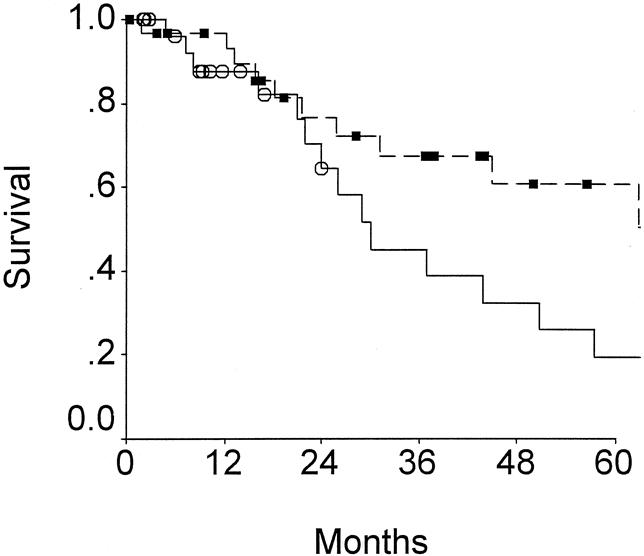
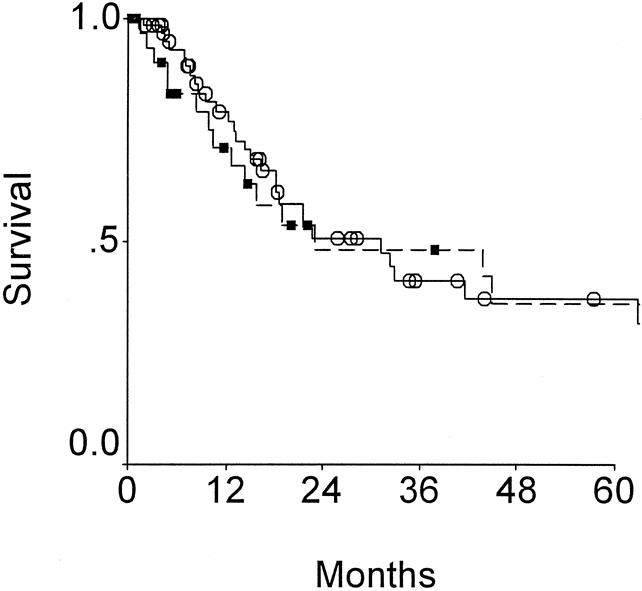
Results: Overall Outcome: 51 patients were inoperable, 92 were subjected to exploration and biopsy only, 135 to noncurative cholecystectomy, 30 to surgical bypass, and 102 to potentially curative resections consisting of portal lymph node dissection and liver parenchymal resections. Operative mortality was 3.9%. T-stage predicted likelihood of distant metastases and resectability. Median survival for resected patients was 26 months and 5-year survival was 38%, and for patients not resected, 5.4 months and 4% (P <.0001). Effect of Prior Operation: 22 patients subjected to potentially curative resection as the first surgical procedure were compared to 80 patients resected after prior exploration elsewhere. Mortality, complication, and long-term survival were the same. By multivariate analysis (Cox regression), resectability and stage were independent predictors (P <.001) of long-term survival, but prior surgical exploration was not.
Conclusion: Unresected gallbladder cancer is a rapidly fatal disease. Radical resection can provide long-term survival, even for large tumors with extensive liver invasion. Long-term survival can be achieved for patients presenting after prior noncurative surgical exploration.
Figures
References
-
- Blalock AA. A statistical study of 888 cases of biliary tract disease. Johns Hopkins Hosp Bull 1924; 35: 391–409.
-
- Piehler JM, Crichlow RW. Primary carcinoma of the gallbladder. Surg Gynecol Obstet 1978; 147: 929–942. - PubMed
-
- Wilkinson DS. Carcinoma of the gall-bladder: an experience and review of the literature [Review]. Austr N Z J Surg 1995; 65: 724–727. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
