

Laparoscopic repair of giant paraesophageal hernia: 100 consecutive cases
- PMID: 10998659
- PMCID: PMC1421193
- DOI: 10.1097/00000658-200010000-00016
Laparoscopic repair of giant paraesophageal hernia: 100 consecutive cases
Abstract
Objective: To summarize the authors' laparoscopic experience for paraesophageal hernia (PEH).
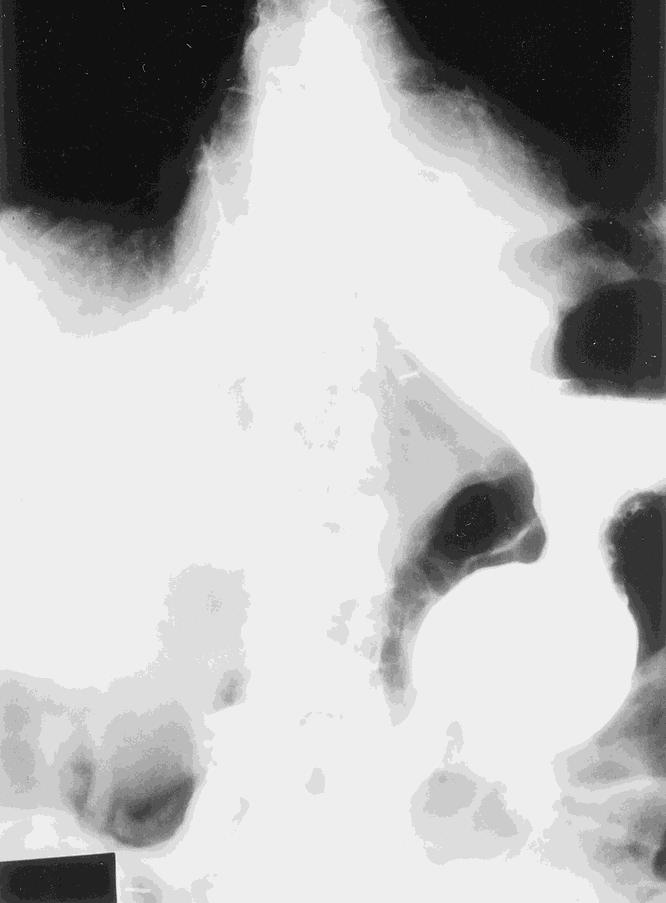
Summary background data: Laparoscopic antireflux surgery and repair of small hiatal hernias are now routinely performed. Repair of a giant PEH is more complex and requires conventional surgery in most centers. Giant PEH accounts for approximately 5% of all hiatal hernias. Medical management may be associated with a 50% progression of symptoms and a significant death rate. Conventional open surgery has a low death rate, but complications are significant and return to routine activities is delayed in this frequently elderly population. Recently, short-term outcome studies have reported that minimally invasive approaches to PEH may be associated with a lower complication rate, a shorter hospital stay, and faster recovery.
Methods: From July 1995 to February 2000, 100 patients (median age 68) underwent laparoscopic repair of a giant PEH. Follow-up included heartburn scores and quality of life measurements using the SF-12 physical component and mental component summary scores.
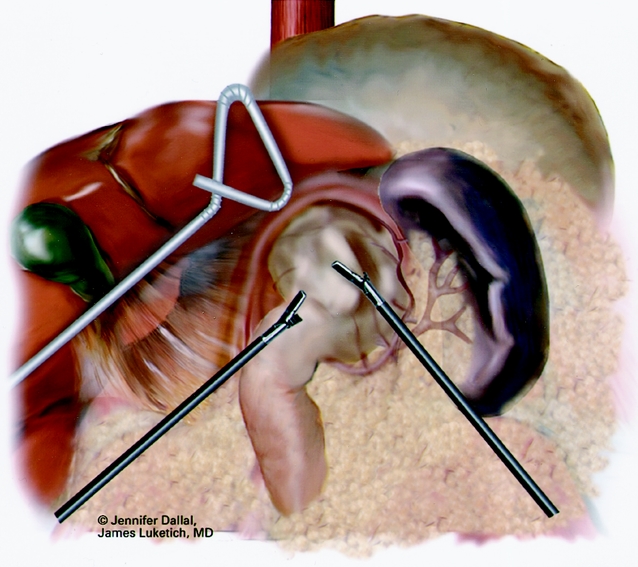
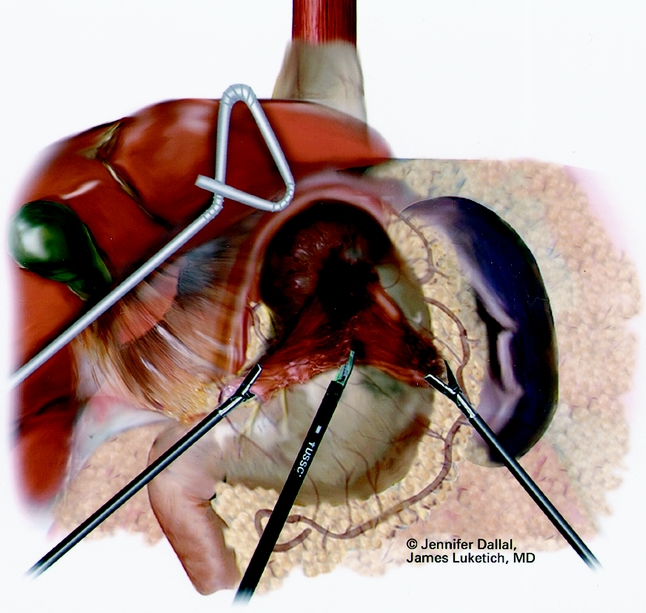
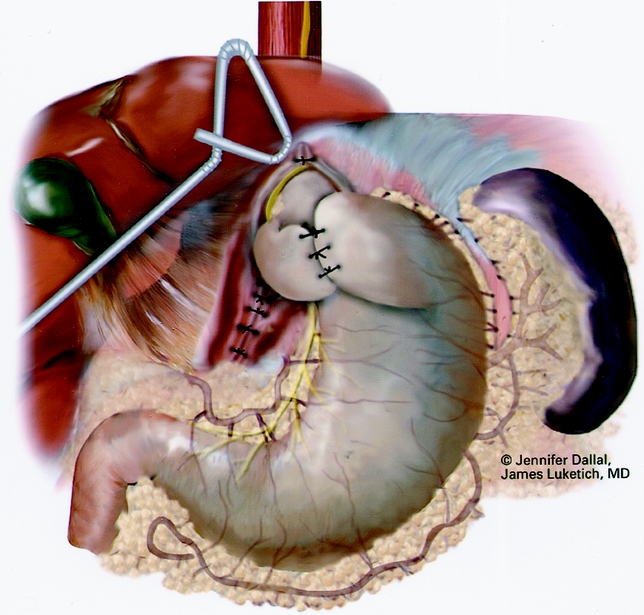
Results: There were 8 type II hernias, 85 type III, and 7 type IV. Sac removal, crural repair, and antireflux procedures were performed (72 Nissen, 27 Collis-Nissen). The 30-day death rate was zero; there was one surgery-related death at 5 months from a perioperative stroke. Intraoperative complications included pneumothorax, esophageal perforation, and gastric perforation. There were three conversions to open surgery. Major postoperative complications included stroke, myocardial infarction, pulmonary emboli, adult respiratory distress syndrome, and repeat operations (two for abscess and one each for hematoma, repair leak, and recurrent hernia). Median length of stay was 2 days. Median follow-up at 12 months revealed resumption of proton pump inhibitors in 10 patients and one repeat operation for recurrence. The mean heartburn score was 2.3 (0, best; 45, worst); the satisfaction score was 91%; physical and mental component summary scores were 49 and 54, respectively (normal, 50).
Conclusion: This report represents the largest series to date of laparoscopic repair of giant PEH. In the authors' center with extensive experience in minimally invasive surgery, laparoscopic repair of giant PEH was successfully performed in 97% of patients, with a minimal complication rate, a 2-day length of stay, and good intermediate results.
Figures


References
-
- Duranceau A, Jamieson GG. Hiatal hernia and gastroesophageal reflux. In: Sabiston DCJ, Lyerly HK, eds. Textbook of surgery. Philadelphia: WB Saunders; 1997: 767–783.
-
- MacArthur KE. Hernias and volvulus of the gastrointestinal tract. In: Feldman M, Scharschmidt BF, Sleisenger MH, Klein S, eds. Sleisenger & Fordtran’s gastrointestinal and liver disease. Philadelphia: WB Saunders; 1998: 318–327.
-
- Haas O, Rat P, Christophe M, Friedman S, Favre JP. Surgical results of intrathoracic gastric volvulus complicating hiatal hernia. Br J Surg 1990; 77: 1379–1381. - PubMed
-
- Treacy PJ, Jamieson GG. An approach to the management of para-oesophageal hiatus hernias. Aust NZ J Surg 1987; 57: 813–817. - PubMed
-
- Skinner DB, Belsey RH. Surgical management of esophageal reflux and hiatus hernia: long-term results with 1,030 patients. J Thorac Cardiovasc Surg 1967; 53: 33–54. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
