

False-negative diffusion-weighted MR findings in acute ischemic stroke
- PMID: 11003275
- PMCID: PMC7974060
False-negative diffusion-weighted MR findings in acute ischemic stroke
Abstract
Background and purpose: Lesions associated with acute stroke are often missed by diffusion-weighted imaging (DWI), suggesting that the sensitivity of this technique for detecting acute ischemic stroke may not be as high as initially thought. Our aim was to estimate the rate of false-negative DWI studies in patients with persistent neurologic deficit due to an ischemic stroke and to identify which stroke lesions are most likely to be missed by DWI.
Methods: We reviewed MR images obtained within 48 hours after stroke onset in 139 patients admitted for symptoms consistent with ischemic stroke in whom the deficit lasted more than 24 hours. Cases of negative initial DWI findings with an ischemic lesion visible on follow-up MR studies and a final diagnosis of arterial ischemic stroke were analyzed in terms of delay between onset of symptoms and initial DWI (MR latency), size and vascular distribution of the lesions, and relationship to findings in patients with positive initial DWI results.
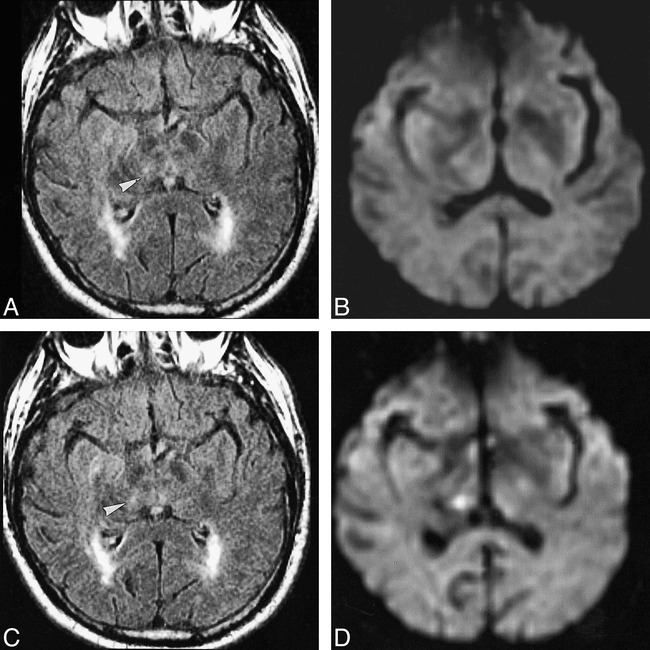
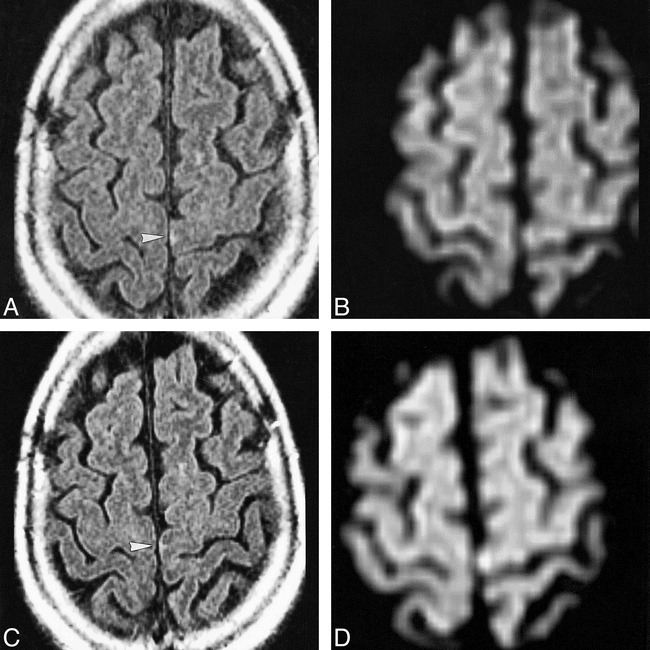
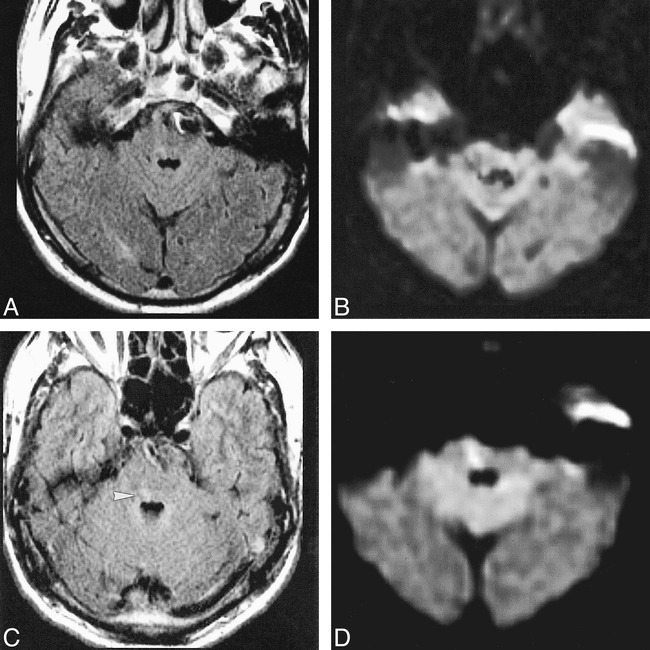
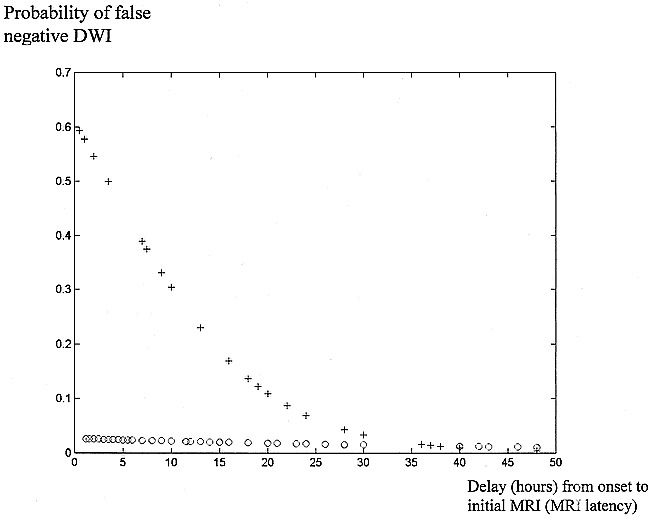
Results: We found eight cases (5.8%) of false-negative initial DWI studies, of which four were positive on initial fluid-attenuated inversion recovery (FLAIR) imaging. Follow-up FLAIR/DWI showed a hyperintensity matching clinical presentation in all eight patients. The mean size of the lesion was 0.19 +/- 0.16 cm3. False-negative studies occurred more often in cases of stroke in the posterior (19%) than in the anterior (2%) circulation or when DWI was obtained within 24 hours after symptom onset. Of the six false-negative vertebrobasilar stroke lesions, five were located in the brain stem. In all, 31% of patients with vertebrobasilar ischemic stroke had a false-negative initial DWI study during the first 24 hours.
Conclusion: A false-negative DWI study is not uncommon during the first 24 hours of ischemic stroke. Vertebrobasilar stroke should therefore not be ruled out on the basis of early negative DWI, especially when symptoms persist and are suggestive of this diagnosis.
Figures
References
-
- Ay H, Buonanno FS, Schaefer PW, et al. Posterior leukoencephalopathy without severe hypertension: utility of diffusion-weighted MRI. Neurology 1998;51:1369-1376 - PubMed
-
- Gonzalez RG, Schaefer PW, Buonanno FS, et al. Diffusion-weighted MR imaging: diagnostic accuracy in patients imaged within 6 hours of stroke symptom onset. Radiology 1999;210:155-162 - PubMed
-
- Le Bihan D, Breton E, Lallemand D, Grenier P, Cabanis E, Laval-Jeantet M. MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders. Radiology 1986;161:401-407 - PubMed
-
- Lutsep HL, Albers GW, DeCrespigny A, Kamat GN, Marks MP, Moseley ME. Clinical utility of diffusion-weighted magnetic resonance imaging in the assessment of ischemic stroke. Ann Neurol 1997;41:574-580 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical