

Case Reports
Colloid cyst of the third ventricle: imaging-pathologic correlation
Affiliations
- PMID: 11003281
- PMCID: PMC7974047
Item in Clipboard
Case Reports
Colloid cyst of the third ventricle: imaging-pathologic correlation
AJNR Am J Neuroradiol.
2000 Sep.
Abstract
Colloid cysts are relatively rare intracranial lesions located in the rostral aspect of the third ventricle. They may produce acute hydrocephalus, brain herniation, and lead to death. Although the clinical and imaging features of colloid cysts are well known, their etiology and the factors responsible for their imaging features continue to be a subject of debate. We present the imaging-pathologic correlation of a patient with a colloid cyst as well as data supporting the fact that the presence of cholesterol is probably responsible for the MR imaging features exhibited by some colloid cysts.
Figures
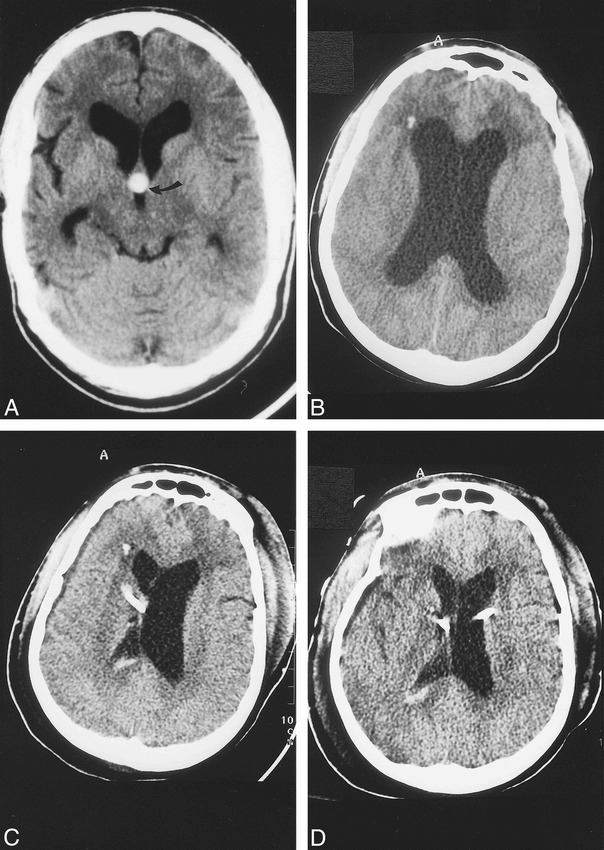
Baseline CT and CT studies obtained during present admission. A, Baseline noncontrast axial 5-mm section shows hyperdense colloid cyst (arrow) in the rostral aspect of the third ventricle. There is moderate dilatation of the lateral ventricles and cerebral atrophy secondary to AIDS. In this view, the colloid cyst is round in appearance. B, CT scan obtained immediately after acute neurologic deterioration shows marked hydrocephalus and hypodensity in the white matter of the frontal lobes. The etiology of the presumed punctate hemorrhage in the right frontal lobe is not known. C, CT obtained immediately after the initial ventriculostomy shows a right-sided catheter that has decompressed the lateral ventricle. The left lateral ventricle remains enlarged and there is mild midline shift to the right. A small amount of blood is present in the right lateral ventricle secondary to catheter insertion. D, CT done after insertion of left-side ventriculostomy shows decreased hydrocephalus, compared with B, and no midline shift.
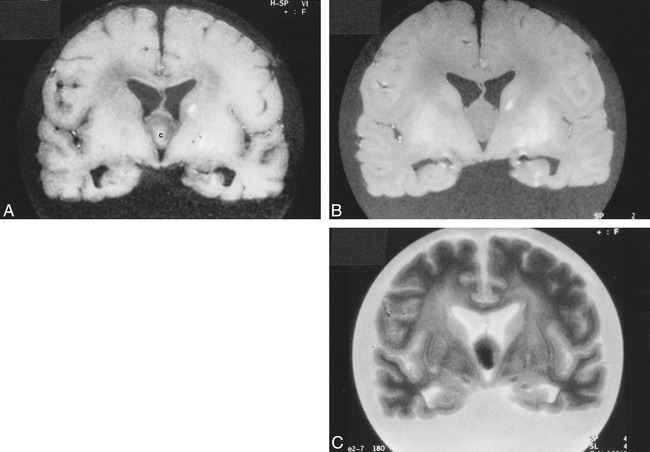
Postmortem MR imaging. A, Coronal T1-weighted image (560/15/1 [TR/TE/excitations]) of the fixed brain shows that the colloid cyst is centrally of higher signal intensity [c] and its rim is relatively hypointense. The lesion is oval-shaped in this projection. The linear hyperintensities in the left basal ganglia are related to a hemorrhagic infarction (see fig 3A). B, Corresponding proton density–weighted image (4500/15/1) shows the lesion to be homogeneous and of similar signal intensity to white matter. C, Corresponding T2-weighted image (4500/105/1) shows the central portion of the cyst to be hypointense and its rim to be slightly hyperintense. Cortical sulci dilatation is well seen in this sequence.
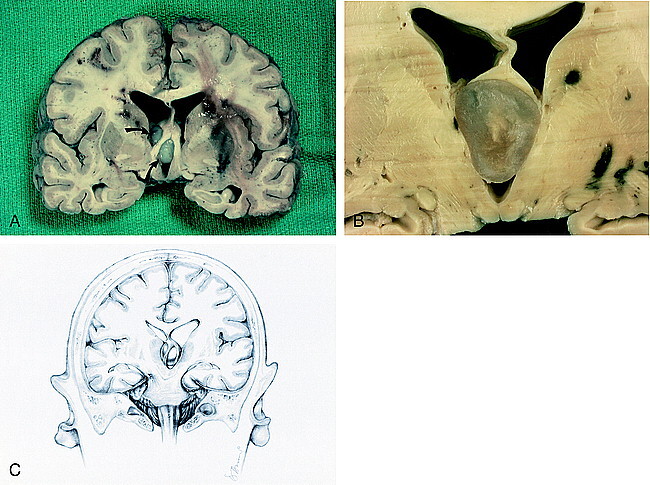
Fixed brain. A, Coronal section shows elevation of the fornices and obstruction of the interventricular foramina of Monro by the colloid cyst (arrows). Bilateral multifocal acute hemorrhages are seen in the periventricular white matter. A hemorrhagic infarction in the left basal ganglia is seen. B, Cut surface of colloid cyst displays turbid, gelatinous material. The fornices are lifted and the third ventricle is expanded. C, Drawing of coronal view shows forniceal columns stradding the colloid cyst wedged in the roof of the third venticle. Note herniation of the left uncus and compression of the contralateral cerebral peduncle against the free edge of the tentorium, causing hemorrhage in the right midbrain.
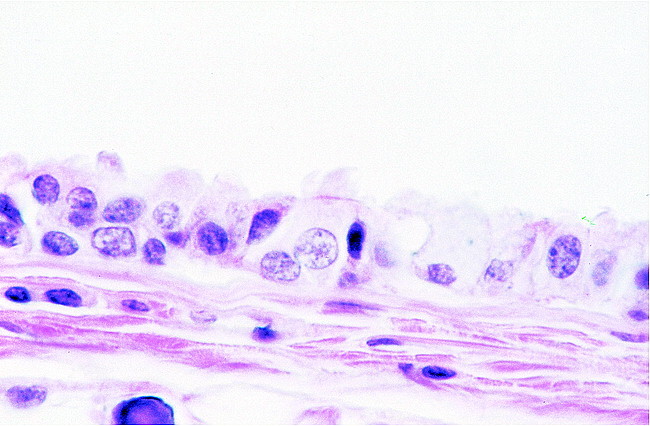
High-power microscopic image. View of the wall of the colloid cyst reveals epithelium with interspersed ciliated and goblet cells resting on collagenous tissue
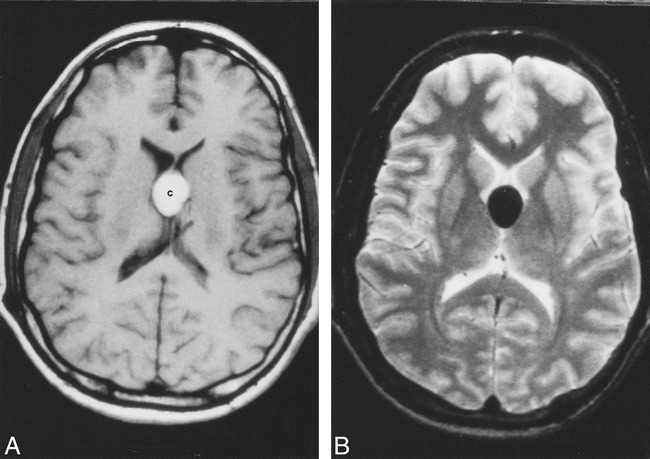
In vivo MR imaging of a colloid cyst (different patient). A, Axial noncontrast T1-weighted image shows oval-shaped, hyperintense colloid cyst [c]. B, Corresponding T2-weighted image shows the cyst to be markedly hypointense. There is no hydrocephalus in this patient.
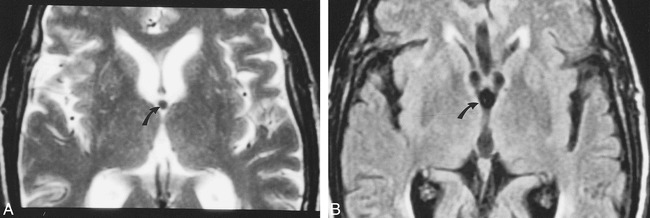
Colloid cyst imaged using FLAIR images (different patient). A, Axial T2-weighted image shows small, rounded, hypointense colloid cyst (arrow) in the anterior aspect of the third ventricle. B, FLAIR image obtained at nearly the same level shows that the colloid cyst (arrow) appears slightly larger than on A and is indistinguishable from the surrounding CSF.
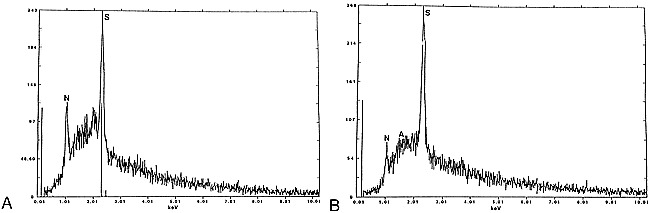
EDX of colloid cysts. A, Analysis of the contents of the entire colloid cyst shown in figs 1–3 shows a large peak (S) corresponding to sulphur, and smaller peaks corresponding to sodium (N) and aluminum (A). B, Analysis of the contents of a different colloid cyst shows large peak (S) of sulphur and also sodium (N). No paramagnetic substances are present in either cyst.
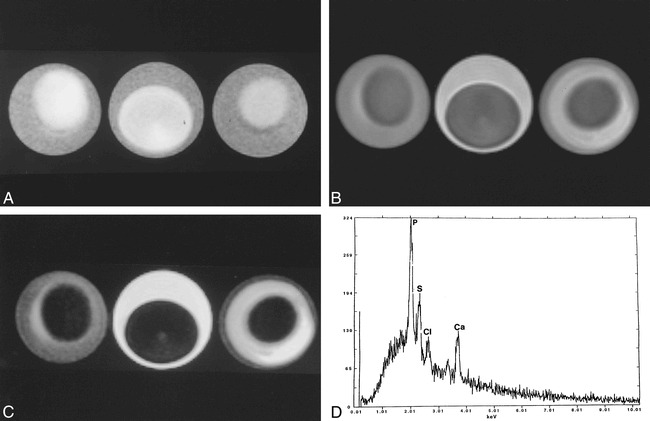
Egg phantom imaged using same parameters as those used for the postmortem brain imaging. A, T1-weighted image of all three eggs (3-minute boiled [left], fresh [middle], and hard boiled [right]) show central relative hyperintensity corresponding to the yolk, the region of higher cholesterol content. The rim (egg white) is relatively hypointense and is probably related to high water content. B, Corresponding proton density–weighted image shows that the yolk is hypointense with respect to the relatively hyperintense egg white. C, Corresponding T2-weighted image shows that the yolk is hypointense with respect to the egg white. The egg white is brighter in the fresh egg and darker on the hard-boiled egg, probably reflecting the amount of free water it contains. The appearance of liquid, semisolid, and solid cholesterol is nearly identical in all sequences. Note that the imaging features of this phantom closely follow those seen in the postmortem study (fig 3) and in some in vivo colloid cysts (fig 5). D, EDX analysis of a hard-boiled egg (mostly yolk) shows sulphur (S), chloride (Cl) and calcium (Ca). The large peak of phosphorus (p) is due to contamination of the yolk by egg white. There are no paramagnetic substances that could be responsible for the appearance of the eggs on MR imaging.
Comment in
-
MR imaging of colloid cysts of the third ventricle.AJNR Am J Neuroradiol. 2001 Sep;22(8):1632. AJNR Am J Neuroradiol. 2001. PMID: 11559521 Free PMC article. No abstract available.
Similar articles
-
Colloid cyst of the third ventricle: sometimes more conspicuous on CT than MR.AJNR Am J Neuroradiol. 1998 May;19(5):875-8. AJNR Am J Neuroradiol. 1998. PMID: 9613503 Free PMC article.
-
Dizygotic twins with a colloid cyst of the third ventricle: case report.Neurosurgery. 2008 Nov;63(5):E1003; discussion E1003. doi: 10.1227/01.NEU.0000330388.91098.89. Neurosurgery. 2008. PMID: 19005365
-
Large hemorrhagic colloid cyst in a 35-year-old male.Turk Neurosurg. 2012;22(6):783-4. doi: 10.5137/1019-5149.JTN.4162-11.1. Turk Neurosurg. 2012. PMID: 23208916
-
Colloid cysts of the third ventricle in identical twins.Br J Neurosurg. 2002 Jun;16(3):303-7. doi: 10.1080/026886902760187604. Br J Neurosurg. 2002. PMID: 12201404 Review.
-
[A case of colloid cyst of the third ventricle].No Shinkei Geka. 1988 Dec;16(13):1483-8. No Shinkei Geka. 1988. PMID: 3067109 Review. Japanese.
Cited by
-
Intracranial lesions with high signal intensity on T1-weighted MR images - review of pathologies.Pol J Radiol. 2013 Oct;78(4):36-46. doi: 10.12659/PJR.889663. Epub 2013 Nov 19. Pol J Radiol. 2013. PMID: 24505222 Free PMC article. Review.
-
Third Ventricle Colloid Cyst as a Cause of Sudden Drop Attacks of a 13-Year-Old Boy.Emerg (Tehran). 2015 Fall;3(4):162-4. Emerg (Tehran). 2015. PMID: 26495408 Free PMC article.
-
The Variable Appearance of Third Ventricular Colloid Cysts: Correlation with Histopathology and the Risk of Obstructive Ventriculomegaly.AJNR Am J Neuroradiol. 2020 Oct;41(10):1833-1840. doi: 10.3174/ajnr.A6722. Epub 2020 Sep 10. AJNR Am J Neuroradiol. 2020. PMID: 32912876 Free PMC article.
-
Imaging of supratentorial intraventricular masses in children: a pictorial review-part 2.Neuroradiology. 2024 May;66(5):699-716. doi: 10.1007/s00234-023-03253-3. Epub 2023 Dec 12. Neuroradiology. 2024. PMID: 38085360 Free PMC article. Review.
-
[Supratentorial tumors].Radiologe. 2007 Jun;47(6):471-85. doi: 10.1007/s00117-007-1519-3. Radiologe. 2007. PMID: 17541538 Review. German.
References
-
- Hernesniemi J, Leivo S. Management outcome in third ventricular colloid cysts in a defined population; a series of 40 patients treated mainly by transcallosal microsurgery. Surg Neurol 1996;45:2-14 - PubMed
-
- Bigner DD, McLendon RE, Bruner JM. Russell and Rubinstein's Pathology of Tumors of the Nervous System. 6th ed. London: Hodder Headline Group 1998;338-342
-
- Zulch KJ. Brain Tumors.. Their Biology and Pathology. 3rd ed. Berlin: Springer-Verlag 1986;519
-
- Macdonald RL, Humphreys RP, Rutka JT, Kestle JRW. Colloid cysts in children. Pediatr Neurosurg 1994;20:169-177 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical