

Leigh syndrome: serial MR imaging and clinical follow-up
- PMID: 11003287
- PMCID: PMC7974045
Leigh syndrome: serial MR imaging and clinical follow-up
Abstract
Background and purpose: Subacute necrotizing encephalomyelopathy, or Leigh syndrome (LS), is a progressive neurodegenerative disorder characterized by symmetrical spongiform lesions in the brain with onset usually in infancy or early childhood. Little is known of the developing process of the brain lesions in LS that are particularly relevant to the occurrence of fatal respiratory failure. Our purpose was to determine whether fatal respiratory failure can be predicted before death on the basis of clinical characteristics or findings on longitudinal MR images of the brain.
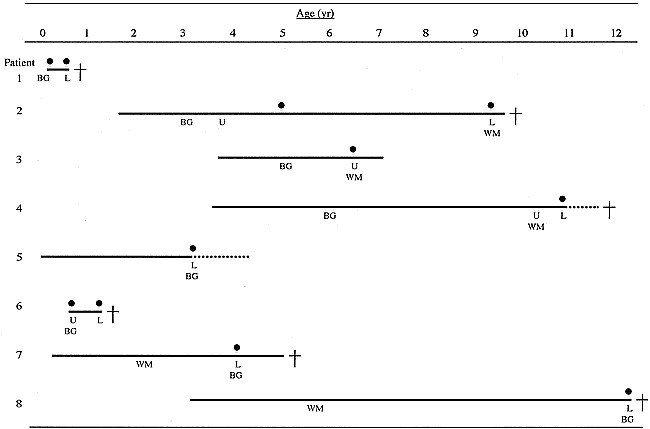
Methods: Clinical records and serial MR studies of eight patients with LS aged 3 months to 12 years who met the diagnostic criteria for LS were reviewed retrospectively, with special reference to a correlation between loss of respiratory control and MR abnormalities. Both T1- and T2-weighted images were obtained at the onset of disease or when clinical symptoms worsened.
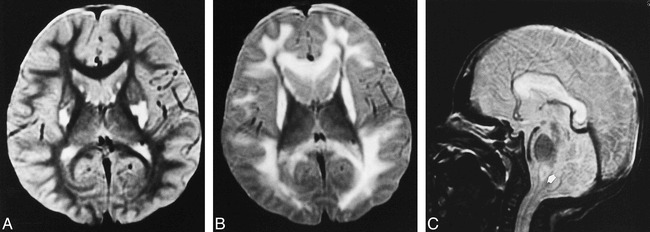
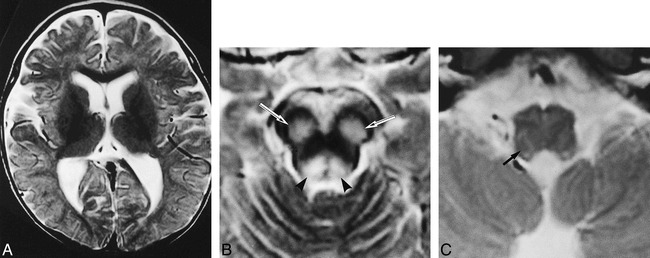
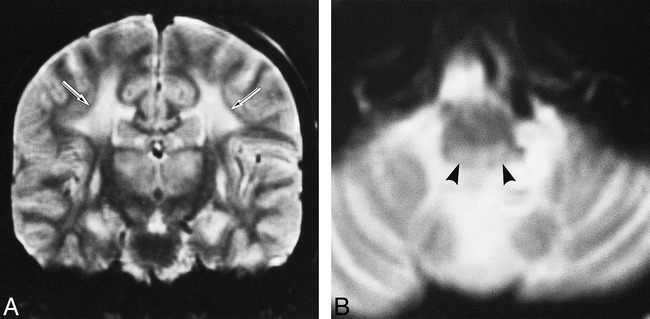
Results: Serial MR images were divided into three groups on the basis of the following findings: 1) symmetrical basal ganglia lesions before brain stem involvement (n = 4); 2) initial involvement of the brain stem (n = 2); and 3) cerebral white matter lesions followed by brain stem lesions (n = 2). Lesions of the lower brain stem were always present when patients had near fatal respiratory failure. However, upper brain stem lesions were transient and were found in parallel to reversible respiratory disorder. Fatal respiratory failure was unpredictable from clinical or neuroradiologic findings.
Conclusion: Brain stem lesions are associated with the loss of respiratory control in patients with LS, but the time at which fatal respiratory failure will occur is unpredictable.
Figures

References
-
- Montpetit VJA, Andermann F, Carpenter S, Fawcett JS, ZborowskaSluis D, Giberson HR. Subacute narcotizing encephalomyelopathy. Brain 1971;94:1-30 - PubMed
-
- Sparaco M, Bonilla E, DiMauro S, Powers J. Neuropathology of mitochondrial encephalomyopathies due to mitochondrial DNA defects. J Neuropathol Exp Neurol 1993;52:1-10 - PubMed
-
- Lyon G, Adams RD, Kolodny EH. Neurology of Hereditary Metabolic Diseases of Children.. New York: McGraw-Hill 1996;94-100
-
- Rahman S. Blok RB, Dahl HHM, et al. Leigh syndrome: clinical features and biochemical and DNA abnormalities. Ann Neurol 1996;39:343-351 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous