

Patient characteristics, diagnosis, and treatment of non-contact lens related Acanthamoeba keratitis
- PMID: 11004092
- PMCID: PMC1723254
- DOI: 10.1136/bjo.84.10.1103
Patient characteristics, diagnosis, and treatment of non-contact lens related Acanthamoeba keratitis
Abstract
Aim: To review the clinical characteristics, diagnosis, and visual outcome in patients with non-contact lens related Acanthamoeba keratitis and compare the findings with reported series of contact lens associated Acanthamoeba keratitis.
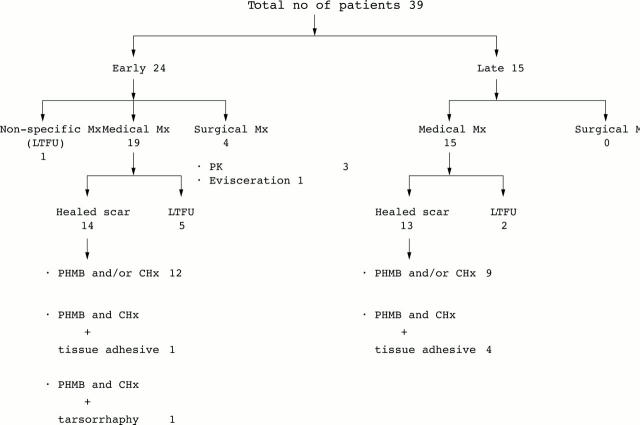
Methods: Medical and microbiology records of 39 consecutive patients with a diagnosis of Acanthamoeba keratitis, at a tertiary eyecare centre in India between January 1996 and June 1998, were analysed retrospectively.
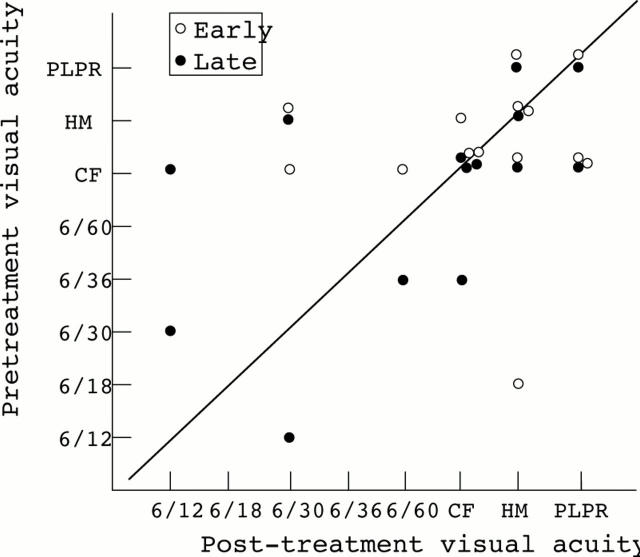
Results: A majority of the patients presented with poor visual acuity and large corneal stromal infiltrates (mean size 38.20 (SD 26. 18) mm). A predisposing factor was elicited in 19/39 (48.7%) patients (trauma 15, dirty water splash three, leaf juice one). None of the patients had worn contact lenses. Most patients (26/39 (66. 6%)) came from a low socioeconomic background. Complaint of severe pain was not a significant feature and radial keratoneuritis was seen in 1/39 (2.5%) patients. A ring infiltrate was present in 41.1% of cases. A clinical diagnosis of fungal keratitis was made in 45% of the patients before they were seen by us. However, all patients were diagnosed microbiologically at our institute based on demonstration of Acanthamoeba cysts in corneal scrapings (34/39) and/or culture of Acanthamoeba (34/39). Treatment with biguanides (PHMB, 15/38 (39.4%), PHMB with CHx, 23/38 (60.5%), one patient did not return for treatment) resulted in healing with scar formation in 27 out of 31(87.0%) followed up patients (mean time to healing 106.9 days). Overall visual outcome was poor with no statistical difference between cases diagnosed within 30 days (early) or 30 days after (late) start of symptoms. The visual outcome in cases requiring tissue adhesive (five) and keratoplasty (three) was also poor.
Conclusions: This is thought to be the largest series of cases of Acanthamoeba keratitis in non-contact lens wearers. In such cases, the disease is advanced at presentation in most patients, pathognomonic clinical features are often not seen, disease progression is rapid, and visual outcome is usually poor. Possible existence of Acanthamoeba pathotypes specifically associated with non-contact lens keratitis and unique to certain geographical areas is suggested.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources