

Fungal and parasitic infections of the eye
- PMID: 11023963
- PMCID: PMC88956
- DOI: 10.1128/CMR.13.4.662
Fungal and parasitic infections of the eye
Abstract
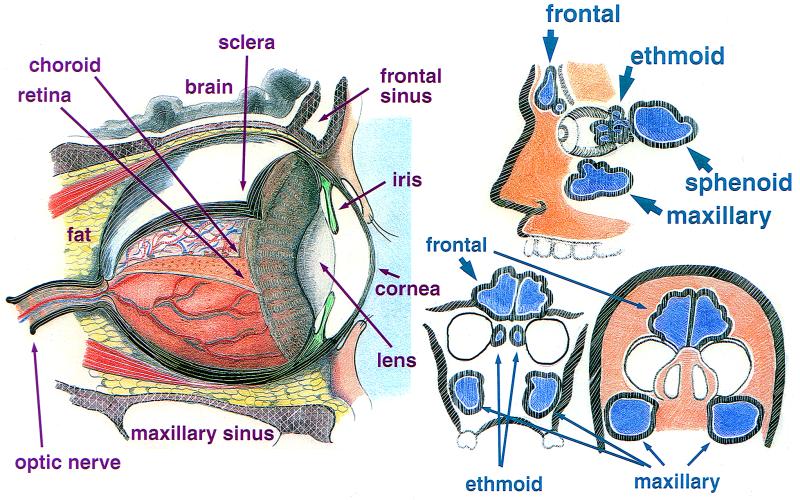
The unique structure of the human eye as well as exposure of the eye directly to the environment renders it vulnerable to a number of uncommon infectious diseases caused by fungi and parasites. Host defenses directed against these microorganisms, once anatomical barriers are breached, are often insufficient to prevent loss of vision. Therefore, the timely identification and treatment of the involved microorganisms are paramount. The anatomy of the eye and its surrounding structures is presented with an emphasis upon the association of the anatomy with specific infection of fungi and parasites. For example, filamentous fungal infections of the eye are usually due to penetrating trauma by objects contaminated by vegetable matter of the cornea or globe or, by extension, of infection from adjacent paranasal sinuses. Fungal endophthalmitis and chorioretinitis, on the other hand, are usually the result of antecedent fungemia seeding the ocular tissue. Candida spp. are the most common cause of endogenous endophthalmitis, although initial infection with the dimorphic fungi may lead to infection and scarring of the chorioretina. Contact lens wear is associated with keratitis caused by yeasts, filamentous fungi, and Acanthamoebae spp. Most parasitic infections of the eye, however, arise following bloodborne carriage of the microorganism to the eye or adjacent structures.
Figures




References
-
- Adams A D. The morphology of human conjunctival mucus. Arch Ophthalmol. 1979;97:730–734. - PubMed
-
- Agger W A. Sporotrichosis. In: Fraunfelder F T, Roy F H, editors. Current ocular therapy. W. B. Philadelphia, Pa: Saunders Company; 1995. pp. 79–80.
-
- Ainbinder D, Parmley V C, Mader T H, Nelson M L. Infectious crystalline keratopathy caused by Candida guilliermondii. Am J Ophthalmol. 1998;125:723–725. - PubMed
-
- Akham O, Bilgi S, Akata D, Kiratli H, Ozmen M. Percutaneous treatment of an orbital hydatic cyst: a new therapeutic approach. Am J Ophthalmol. 1998;125:827–829. - PubMed
-
- Akler M, Vellend H, McNeely D M, Walmsley S L, Gold W L. Use of fluconazole in the treatment of candidal endophthalmitis. Clin Infect Dis. 1995;20:657–664. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
