

Carotid artery stenting: technical considerations
- PMID: 11039358
- PMCID: PMC8174855
Carotid artery stenting: technical considerations
Abstract
Background and purpose: Carotid endarterectomy (CEA) is one of the most frequently performed operations in the United States. To offer patients a less invasive means to achieve the same goal, carotid artery stenting (CAS) is investigated as an alternative treatment to CEA.
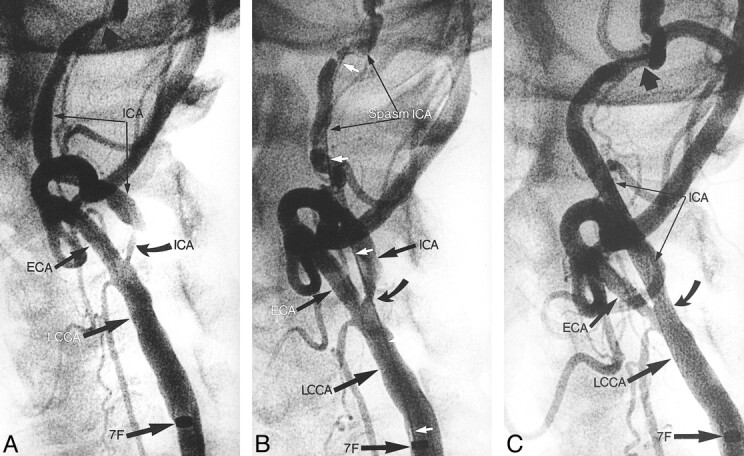
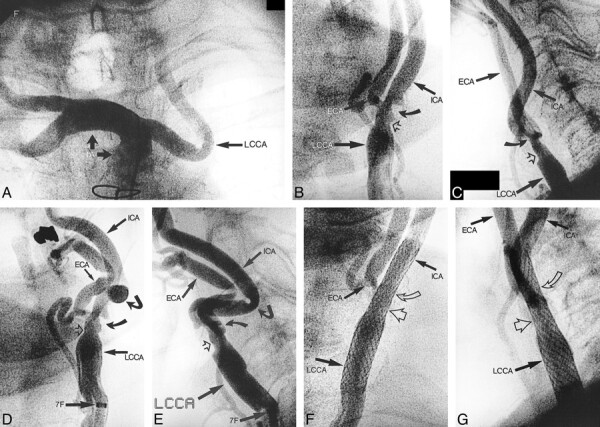
Methods: Three hundred ninety patients underwent CAS, with 451 vessels treated. CAS was performed using a coaxial system with a 7F 90-cm sheath for predilation, stent placement, and stent dilation. Pretreatment antiplatelet therapy was administered. We currently practice same-day admissions and 23-hour discharges.
Results: The technical success rate was 98%. The 30-day mortality/morbidity rates were as follows: death, 1.7% (two [0.5%] neurologic and five [1.2%] systemic] major strokes, 0.9% (two of four were related to the intervention); minor strokes, 5.5%. Among 25 patients who suffered minor strokes, 14 achieved complete recovery. On an annual basis, the incidence of minor stroke declined from 6.8% (1994-1995), to 5.8% (1995-1996), 5.3% (1996-1997), and then 4% (1997-1998), with no major strokes or neurologic deaths occurring during the 1997 to 1998 period.
Conclusion: CAS is an effective treatment for carotid stenosis. With proper selection of patients and meticulous technique, complication rates compare favorably with those of CEA.
Figures
References
-
- Mathias K. Stent placement in supra-aortic artery disease. In: Liermann DD, ed. Stents: State of the Art and Future Developments. Morin Heights: Polyscience Publication, Inc. 1995;87-92
-
- Diethrich EB, Ndiaye M, Reid DB. Stenting in the carotid artery: initial experience in 110 patients. J Endovasc Surg 1996;3:42-62 - PubMed
-
- Roubin GS, Yadav JS, Iyer SS, Vitek JJ. Carotid stent supported angioplasty: a neurovascular intervention to prevent stroke. Am J Cardiol 1996;78:8-12 - PubMed
-
- Théron JG, Payelle GG, Coskun O, Huet HF, Guimaraens L. Carotid artery stenosis: treatment with protected balloon angioplasty and stent placement. Radiology 1996;201:627-636 - PubMed
-
- Wholey MH, Wholey M, Bergeron P, et al. Current global status of carotid artery stent placement. Cath Cardiovasc Diagn 1998;44:1-6 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources