

Contrast enhanced electron beam computed tomography to analyse the coronary arteries in patients after acute myocardial infarction
- PMID: 11040005
- PMCID: PMC1729467
- DOI: 10.1136/heart.84.5.489
Contrast enhanced electron beam computed tomography to analyse the coronary arteries in patients after acute myocardial infarction
Abstract
Objective: To evaluate the accuracy of contrast enhanced electron beam computed tomography (EBCT) after acute myocardial infarction in determining patency of the infarct related artery and detecting high grade stenoses and occlusions in the coronary vessels.
Design: Case study using blinded comparison with invasive coronary angiography.
Patients: 36 patients (mean age 53 years) 4-70 days after acute myocardial infarction.
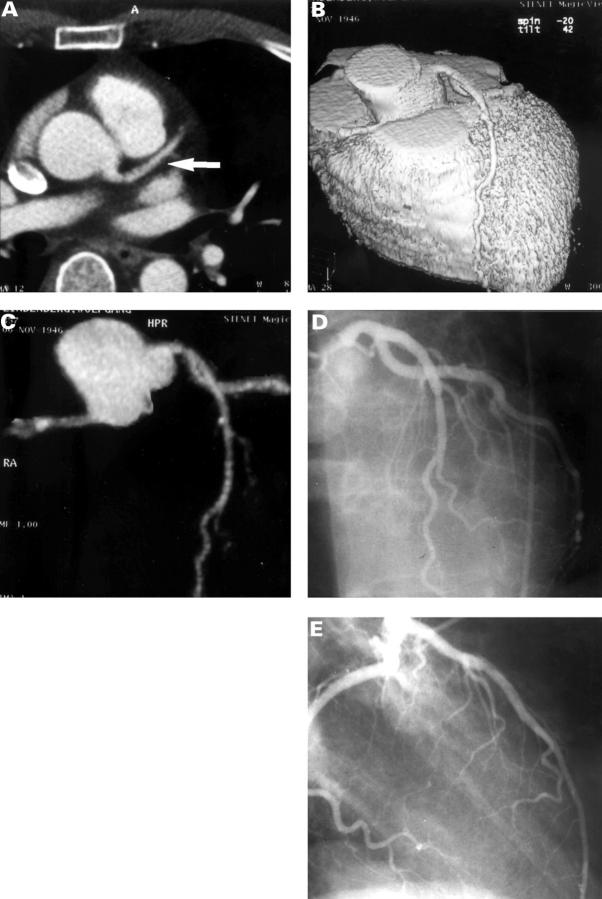
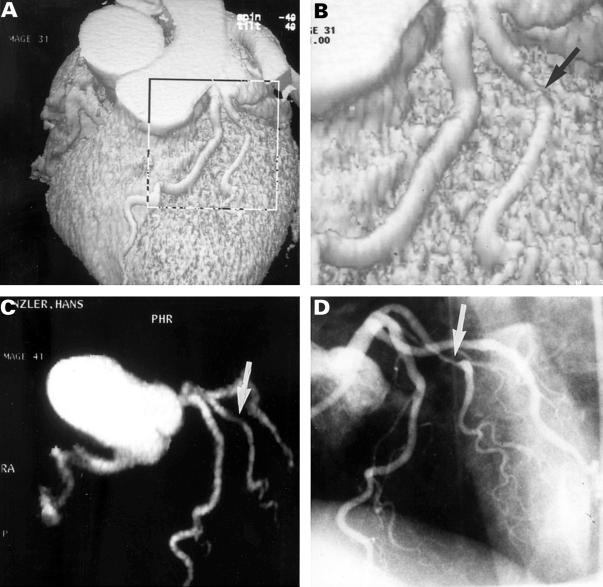
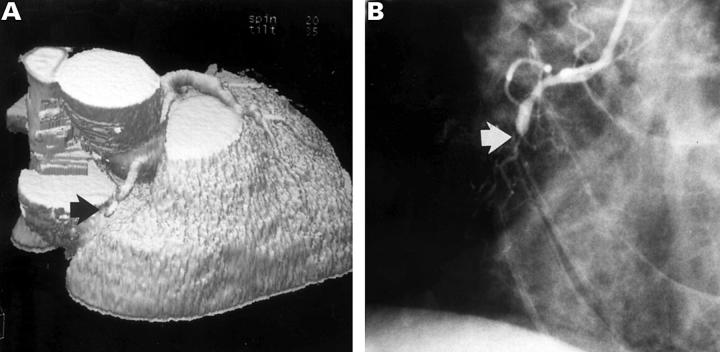
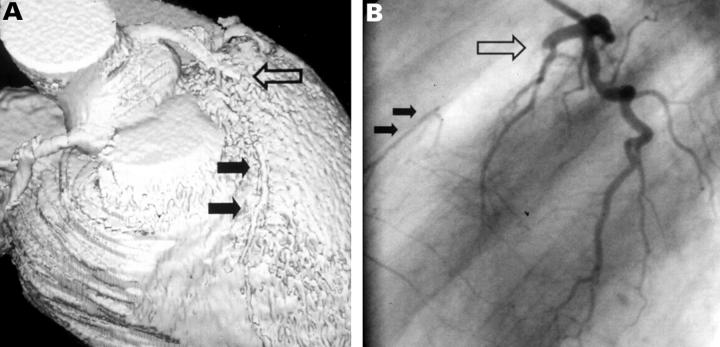
Interventions: The patients were studied by EBCT and invasive coronary angiography. For EBCT, 50 axial images of the heart (3 mm slice thickness) were acquired. They were triggered by the ECG during breath holding, after intravenous injection of contrast agent. The original images, surface reconstructions, and maximum intensity projections were evaluated for the presence of high grade stenoses and occlusions of the coronary arteries.
Main outcome measures: EBCT results were compared with invasive coronary angiography.
Results: Of a total of 144 coronary arteries (left main, left anterior descending, left circumflex, and right coronary artery in 36 patients), 29 (20%) were unevaluable by EBCT. In the remaining arteries, 33 of 36 high grade lesions were correctly detected (92% sensitivity). Specificity was also 92% (73/79). Patency of the infarct related artery was correctly detected in 15 of 16 cases (94%). Five of the 14 occluded infarct related arteries (35%) were mistaken as stenotic but patent, and six could not be assessed.
Conclusions: EBCT is very accurate in detecting significant coronary artery lesions in patients after acute myocardial infarction, but differentiation between occluded and patent infarct related arteries is currently unreliable.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical