

Frequency of oestrogen and progesterone receptor positivity by immunohistochemical analysis in 7016 breast carcinomas: correlation with patient age, assay sensitivity, threshold value, and mammographic screening
- PMID: 11041059
- PMCID: PMC1731243
- DOI: 10.1136/jcp.53.9.688
Frequency of oestrogen and progesterone receptor positivity by immunohistochemical analysis in 7016 breast carcinomas: correlation with patient age, assay sensitivity, threshold value, and mammographic screening
Abstract
Aims: A routine immunohistochemical (IHC) assay is now commonly used for determining the oestrogen receptor (ER) and progesterone receptor (PR) status of women with breast cancer. To date, no large studies have been conducted that report the expected frequency of receptor positivity in relation to patient age and sensitivity of the IHC assay. Data on 7016 breast carcinomas from 71 laboratories were analysed to determine the frequency of receptor positivity and investigate possible causes of the observed variation in detection rates.
Methods: Members of UK NEQAS-ICC (UK National External Quality Assessment Scheme for Immunocytochemistry) provided data on the receptor status of cases routinely assayed in their departments over a period of two to 26 months between June 1996 and September 1998. Data on 7016 breast carcinomas were stratified according to patient age and receptor status. Frequency of receptor positivity was correlated with IHC assay sensitivity, the threshold value used to determine receptor positivity, and the presence or absence of mammographic screening in the hospitals or clinics served by the laboratories.
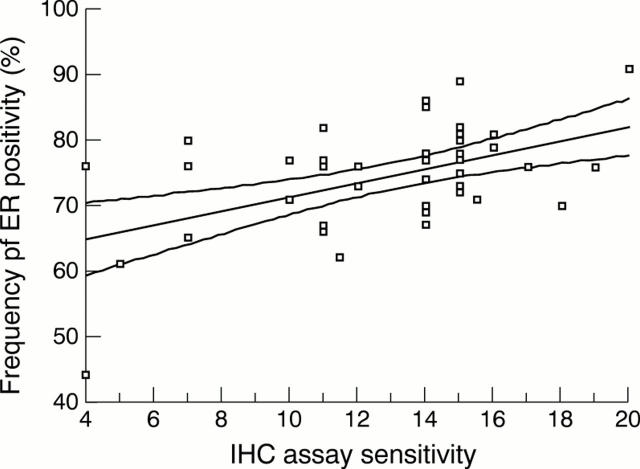
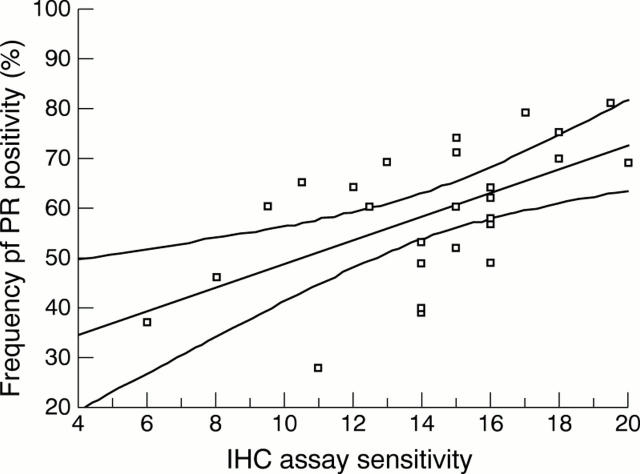
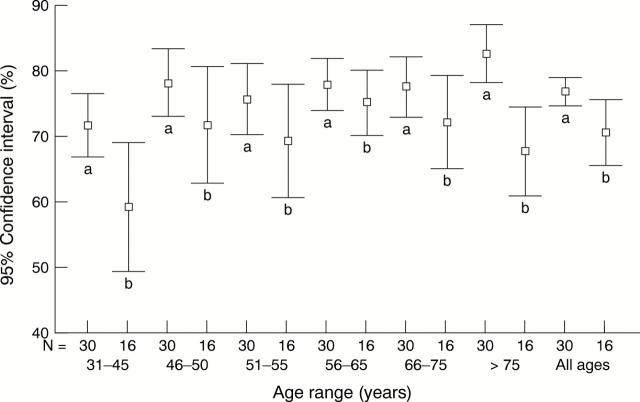
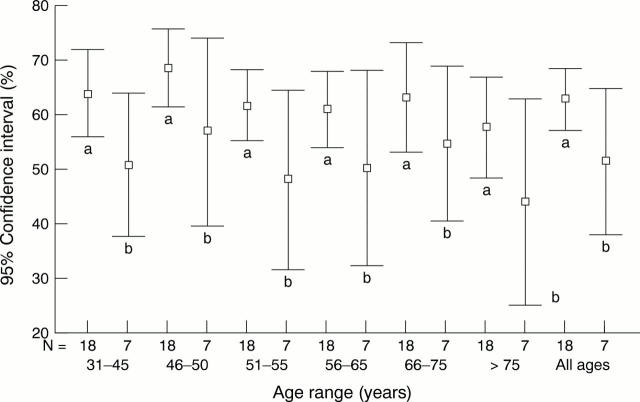
Results: The highest proportion of receptor positive cases occurred in patients in the age ranges > 65 years for ER and 41-50 years for PR. There was a significant positive correlation between frequency of receptor positivity and the sensitivity of the IHC assay, for both ER (rs = 0.346; p = 0.019; two tailed) and PR (rs = 0.561; p = 0.003; two tailed). The mean frequency of receptor positivity for laboratories using the same 10% threshold value was 77% for ER (95% confidence interval (CI), 74% to 80%) in laboratories with high sensitivity and 72% (95% CI, 68% to 76%) for those with low assay sensitivity (p = 0.025). For PR, the mean frequency of receptor positivity for laboratories using the same 10% threshold value and having high assay sensitivity was 63% (95% CI, 57% to 69%), and 51% (95% CI, 38% to 65%) for laboratories with assays of low sensitivity (p = 0.022). The mean frequency of ER positivity for laboratories serving hospitals and clinics where mammographic screening does and does not take place was 73.4% and 75.7%, respectively (p = 0.302; two tailed).
Conclusions: Of the parameters investigated, patient age and IHC assay sensitivity were found to be the main variables influencing the frequency of receptor positivity. We recommend the range of receptor values obtained by laboratories achieving high assay sensitivity as a useful guide against which all laboratories can gauge their own results.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials