

Randomised controlled trial of midwife led debriefing to reduce maternal depression after operative childbirth
- PMID: 11053173
- PMCID: PMC27510
- DOI: 10.1136/bmj.321.7268.1043
Randomised controlled trial of midwife led debriefing to reduce maternal depression after operative childbirth
Abstract
Objective: To assess the effectiveness of a midwife led debriefing session during the postpartum hospital stay in reducing the prevalence of maternal depression at six months postpartum among women giving birth by caesarean section, forceps, or vacuum extraction.
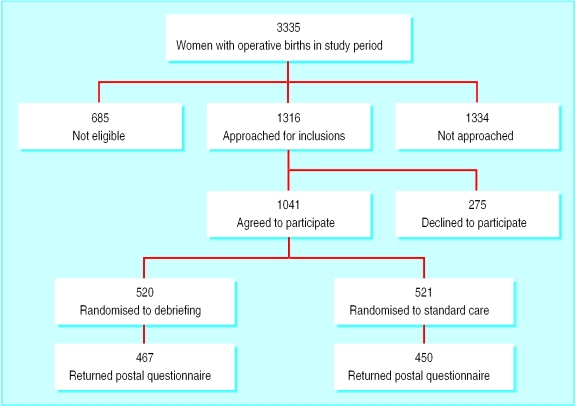
Design: Randomised controlled trial.
Setting: Large maternity teaching hospital in Melbourne, Australia.
Participants: 1041 women who had given birth by caesarean section (n= 624) or with the use of forceps (n= 353) or vacuum extraction (n= 64).
Main outcome measures: Maternal depression (score >/=13 on the Edinburgh postnatal depression scale) and overall health status (comparison of mean scores on SF-36 subscales) measured by postal questionnaire at six months postpartum.
Results: 917 (88%) of the women recruited responded to the outcome questionnaire. More women allocated to debriefing scored as depressed six months after birth than women allocated to usual postpartum care (81 (17%) v 65 (14%)), although this difference was not significant (odds ratio=1.24, 95% confidence interval 0.87 to 1.77). They were also more likely to report that depression had been a problem for them since the birth, but the difference was not significant (123 (28%) v 94 (22%); odds ratio=1. 37, 1.00 to 1.86). Women allocated to debriefing had poorer health status on seven of the eight SF-36 subscales, although the difference was significant only for role functioning (emotional): mean scores 73.32 v 78.98, t= -2.31, 95% confidence interval -10.48 to -0.84).
Conclusions: Midwife led debriefing after operative birth is ineffective in reducing maternal morbidity at six months postpartum. The possibility that debriefing contributed to emotional health problems for some women cannot be excluded.
Figures
Comment in
- ACP J Club. 2001 May-Jun;134(3):86
-
The current status of psychological debriefing.BMJ. 2000 Oct 28;321(7268):1032-3. doi: 10.1136/bmj.321.7268.1032. BMJ. 2000. PMID: 11053152 Free PMC article. No abstract available.
-
Midwife led debriefing to reduce maternal depression. Effectiveness of individual midwives is unclear.BMJ. 2000 Dec 9;321(7274):1470. doi: 10.1136/bmj.321.7274.1470. BMJ. 2000. PMID: 11187945 Free PMC article. No abstract available.
-
Psychological debriefing. Qualitative research may be more appropriate.BMJ. 2001 Apr 14;322(7291):929. BMJ. 2001. PMID: 11302913 No abstract available.
-
Psychological debriefing. Providing good clinical care means listening to women's concerns.BMJ. 2001 Apr 14;322(7291):928. BMJ. 2001. PMID: 11302918 Free PMC article. No abstract available.
-
Psychological debriefing. Research methodology was inadequate.BMJ. 2001 Apr 14;322(7291):928; author reply 929. BMJ. 2001. PMID: 11302920 No abstract available.
References
-
- Brown S, Lumley J. Maternal health after childbirth: results of an Australian population based survey. Br J Obstet Gynaecol. 1998;105:156–161. - PubMed
-
- Astbury J, Brown S, Lumley J, Small R. Birth events, birth experiences and social factors in depression after birth. Aust J Public Health. 1994;18:176–184. - PubMed
-
- Hillan EM. Short-term morbidity associated with caesarean delivery. Birth. 1992;19:190–194. - PubMed
-
- MacArthur C, Lewis M, Knox EG. Health after childbirth. Br J Obstet Gynaecol. 1991;98:1193–1204. - PubMed
-
- Fisher J, Stanley R, Burrows G. Psychological adjustment to caesarean delivery: a review of the evidence. J Psychosom Obstet Gynaecol. 1990;11:91–106.