

Minimizing charges associated with the determination of brain death
- PMID: 11056697
- PMCID: PMC28989
- DOI: 10.1186/cc105
Minimizing charges associated with the determination of brain death
Abstract
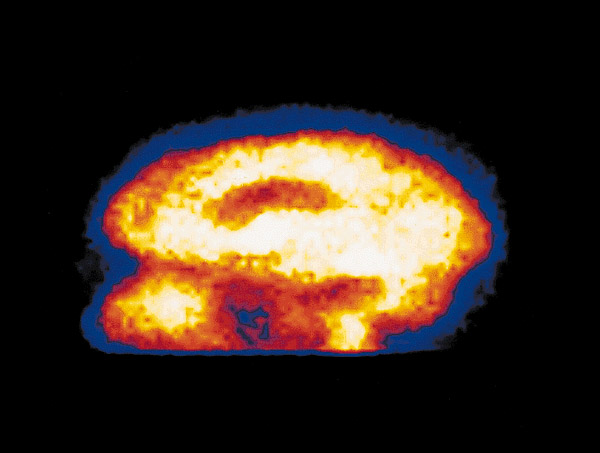
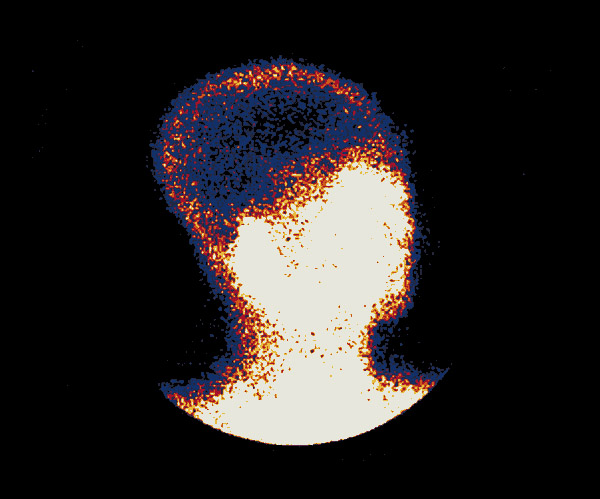
BACKGROUND: The purpose of this study was to evaluate the effect of altering the use of the protocol for brain death determination in traumatically injured patients, on time to brain death determination, medical complication rates, organ procurement rates and charges for care rendered during brain death determination. A retrospective chart review of trauma patients with lethal brain injuries at an urban tertiary care trauma center was performed. Two groups of trauma patients with lethal head injuries were compared. Group I consisted of patients pronounced brain dead using a protocol requiring two brain examinations, and group II contained patients evaluated using a protocol requiring one brain examination in conjunction with a nuclear medicine brain flow scan. RESULTS: Group II had a significantly (P < 0.01) shorter mean brain death stay (3.5 +/- 1.8 h) than group I (12.0 +/- 1.0 h). Patients in groups I and II developed a similar number of medical complications, 3.2 +/- 0.2 and 4.0 +/- 1.3, respectively. The number of organs procured per patient did not differ significantly (4.1 +/- 0.2 for group I and 4.4 +/- 1.4 for group II). There was a significant (P < 0.01) decrease in the brain death stay charges for group II ($6125 +/- 1100) compared to group I ($16,645 +/- 1223). CONCLUSIONS: Medical complications are universal in the traumatized patient awaiting the determination of brain death. These complications necessitate aggressive and costly care in the intensive care unit in order to optimize organ function in preparation for possible transplantation. In our institution, the determination of brain death using a single clinical examination and a nuclear medicine flow study significantly shortened the brain death stay and reduced associated charges accrued during this period. The complication and organ procurement rates were not affected in this small, preliminary report sample.
Figures
References
-
- UNOS 1996 Annual Report: http:www.unos.orgunos_ar_97tab_cont.htm
-
- Stuart FP. Need, supply and legal issues related to organ transplantation in the United States. Transplant Proc. 1984;16:87–94.
-
- Evans RW, Manninen DL, Garrison LP, et al. Donor availability as the primary determinant of the future of heart transplantation. JAMA. 1986;255:1892–1898. - PubMed
-
- Merz B. The organ procurement problem: many causes, no easy solutions. JAMA. 1985;254:3285–3288. - PubMed
-
- Peters TG. Life or death: the issue of payment in cadaveric organ donation. JAMA. 1991;265:1302–1305. - PubMed
LinkOut - more resources
Full Text Sources
