

Variation in red cell transfusion practice in the intensive care unit: a multicentre cohort study
- PMID: 11056725
- PMCID: PMC29015
- DOI: 10.1186/cc310
Variation in red cell transfusion practice in the intensive care unit: a multicentre cohort study
Abstract
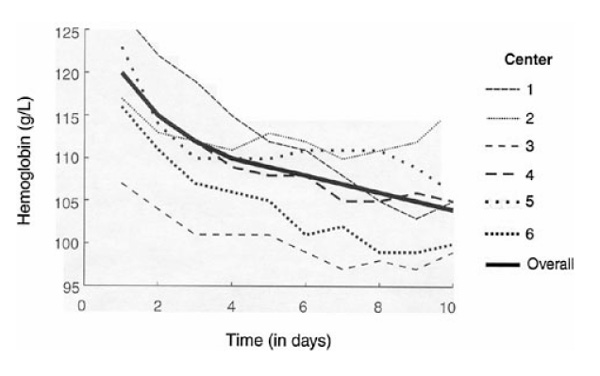
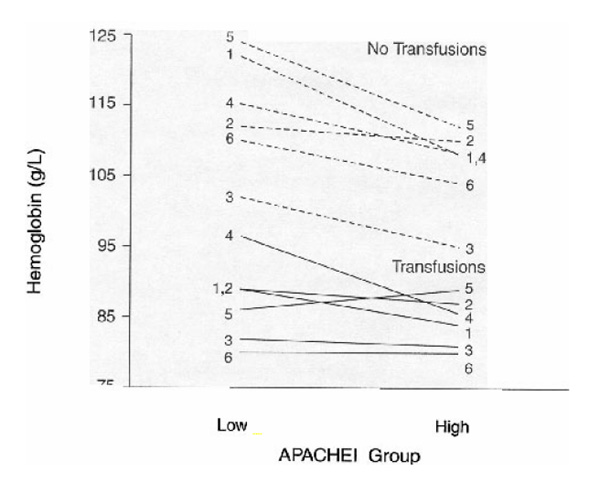
OBJECTIVES: To determine the degree of interinstitutional transfusion practice variation and reasons why red cells are administered in critically ill patients. STUDY DESIGN: Multicentre cohort study combined with a cross-sectional survey of physicians requesting red cell transfusions for patients in the cohort. STUDY POPULATION: The cohort included 5298 consecutive patients admitted to six tertiary level intensive care units in addition to administering a survey to 223 physicians requesting red cell transfusions in these units. MEASUREMENTS: Haemoglobin concentrations were collected, along with the number and reasons for red cell transfusions plus demographic, diagnostic, disease severity (APACHE II score), intensive care unit (ICU) mortality and lengths of stay in the ICU. RESULTS: Twenty five per cent of the critically ill patients in the cohort study received red cell transfusions. The overall number of transfusions per patient-day in the ICU averaged 0.95 +/- 1.39 and ranged from 0.82 +/- 1.69 to 1.08 +/- 1.27 between institutions (P < 0.001). Independent predictors of transfusion thresholds (pre-transfusion haemoglobin concentrations) included patient age, admission APACHE II score and the institution (P < 0.0001). A very significant institution effect (P < 0.0001) persisted even after multivariate adjustments for age, APACHE II score and within four diagnostic categories (cardiovascular disease, respiratory failure, major surgery and trauma) (P < 0.0001). The evaluation of transfusion practice using the bedside survey documented that 35% (202 of 576) of pre-transfusion haemoglobin concentrations were in the range of 95-105 g/l and 80% of the orders were for two packed cell units. The most frequent reasons for administering red cells were acute bleeding (35%) and the augmentation of O2 delivery (25%). CONCLUSIONS: There is significant institutional variation in critical care transfusion practice, many intensivists adhering to a 100g/l threshold, and opting to administer multiple units despite published guidelines to the contrary. There is a need for prospective studies to define optimal practice in the critically ill.
Figures
References
-
- Adams RC, Lundy JS. Anesthesia in cases of poor surgical risk: some suggestions for decreasing the risk. Surg Gynecol Obstet. 1941;71:1011–1014.
-
- Welch HG, Meehan KR, Goodnough LT. Prudent strategies for elective red blood cell transfusion. Ann Intern Med. 1992;116:393–402. - PubMed
-
- Zauder HL. Preoperative hemoglobin requirements. Anesth Clin N Am. 1990;8:471–480.
-
- American College of Physicians Practice strategies for elective red blood cell transfusion. Ann Intern Med. 1992;116:403–406. - PubMed
-
- Silberstein LE, Kruskall MS, Stehling LC, et al. Strategies for the review of transfusion practices. JAMA . 1989;262:1993–1997. - PubMed
LinkOut - more resources
Full Text Sources
