

Human T-cell lymphotropic virus type 1 gag indeterminate western blot patterns in Central Africa: relationship to Plasmodium falciparum infection
- PMID: 11060067
- PMCID: PMC87540
- DOI: 10.1128/JCM.38.11.4049-4057.2000
Human T-cell lymphotropic virus type 1 gag indeterminate western blot patterns in Central Africa: relationship to Plasmodium falciparum infection
Abstract
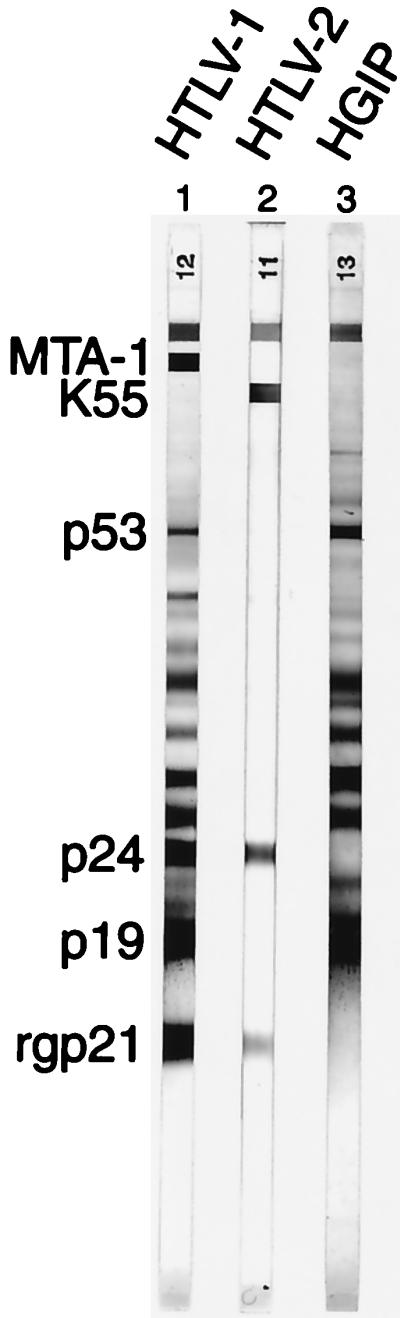
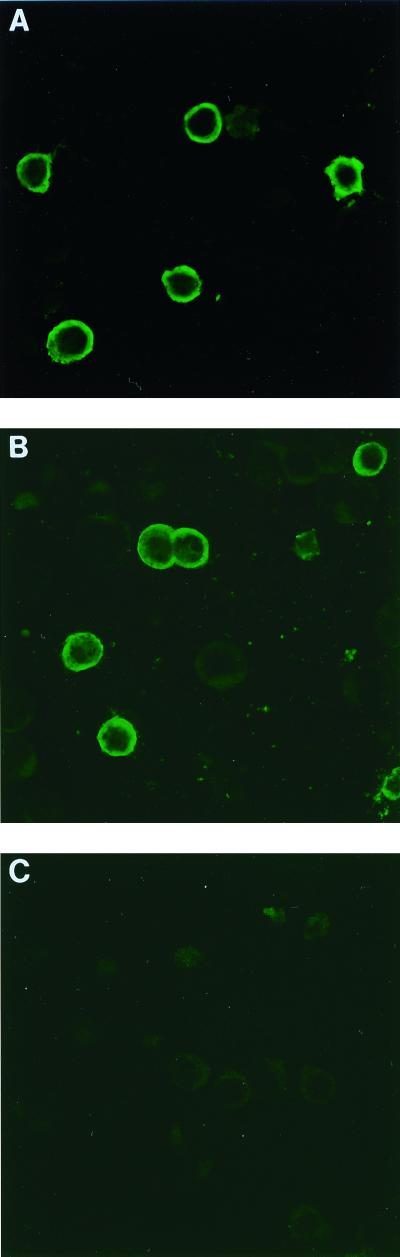
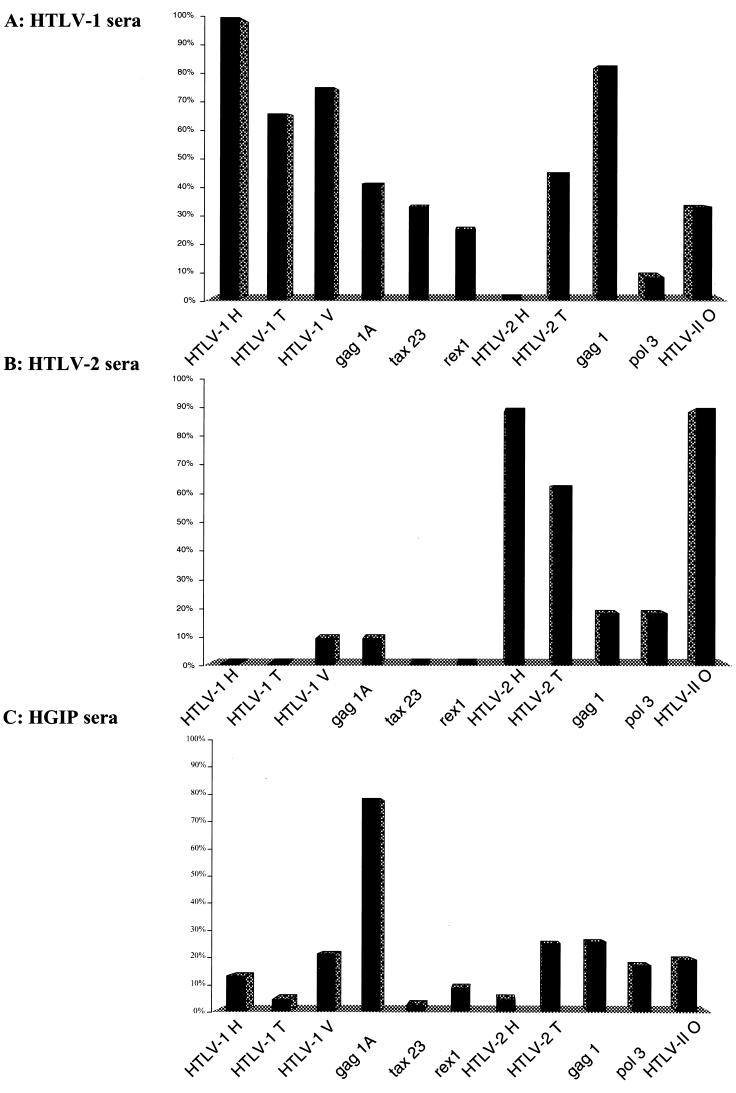
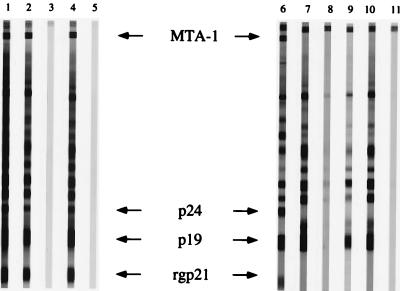
To gain insight on the significance of human T-cell lymphotropic virus type 1 (HTLV-1) indeterminate serological reactivities, we studied villagers of South Cameroon, focusing on a frequent and specific HTLV-1 Gag indeterminate profile (HGIP) pattern (gag p19, p26, p28, and p30 without p24 or Env gp21 and gp46). Among the 102 sera studied, 29 from all age groups had a stable HGIP pattern over a period of 4 years. There was no epidemiological evidence for sexual or vertical transmission of HGIP. Seventy-five percent of HGIP sera reacted positively on MT2 HTLV-1-infected cells by immunofluorescence assay. However, we could not isolate any HTLV-1 virus or detect the presence of p19 Gag protein in cultures of peripheral blood mononuclear cells obtained from individuals with strong HGIP reactivity. PCR experiments conducted with primers for HTLV-1 and HTLV-2 (HTLV-1/2 primers) encompassing different regions of the virus did not yield HTLV-1/2 proviral sequences from individuals with HGIP. Using 11 peptides corresponding to HTLV-1 or HTLV-2 immunodominant B epitopes in an enzyme-linked immunosorbent assay, one epitope corresponding to the Gag p19 carboxyl terminus was identified in 75% of HGIP sera, while it was recognized by only 41% of confirmed HTLV-1-positive sera. A positive correlation between HTLV-1 optical density values and titers of antibody to Plasmodium falciparum was also demonstrated. Finally, passage of sera through a P. falciparum-infected erythrocyte-coupled column was shown to specifically abrogate HGIP reactivity but not the HTLV-1 pattern, suggesting the existence of cross-reactivity between HTLV-1 Gag proteins and malaria-derived antigens. These data suggest that in Central Africa, this frequent and specific Western blot is not caused by HTLV-1 infection but could instead be associated with P. falciparum infection.
Figures
References
-
- Anonymous. Acquired immunodeficiency syndrome (AIDS). Proposed WHO criteria for interpreting results from western blot assays for HIV-1, HIV-2, and HTLV-I/HTLV-II. Wkly Epidemiol Rec. 1990;65:281–283. - PubMed
-
- Anonymous. Seroepidemiology of the human T-cell leukaemia/lymphoma viruses in Europe. The HTLV European Research Network. J Acquir Immune Defic Syndr Hum Retrovirol. 1996;13:68–77. - PubMed
-
- Asher D M, Goudsmit J, Pomeroy K L, Garruto R M, Bakker M, Ono S G, Elliot N, Harris K, Askins H, Eldadah Z, et al. Antibodies to HTLV-I in populations of the southwestern Pacific. J Med Virol. 1988;26:339–351. - PubMed
-
- Banki K, Maceda J, Hurley E, Ablonczy E, Mattson D H, Szegedy L, Hung C, Perl A. Human T-cell lymphotropic virus (HTLV)-related endogenous sequence, HRES-1, encodes a 28-kDa protein: a possible autoantigen for HTLV-I gag-reactive autoantibodies. Proc Natl Acad Sci USA. 1992;89:1939–1943. - PMC - PubMed
-
- Biggar R J, Gigase P L, Melbye M, Kestens L, Sarin P S, Bodner A J, Demedts P, Stevens W J, Paluku L, Delacollette C, et al. ELISA HTLV retrovirus antibody reactivity associated with malaria and immune complexes in healthy Africans. Lancet. 1985;2:520–523. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
