

Richter's hernia and Sir Frederick Treves: an original clinical experience, review, and historical overview
- PMID: 11066144
- PMCID: PMC1421226
- DOI: 10.1097/00000658-200011000-00014
Richter's hernia and Sir Frederick Treves: an original clinical experience, review, and historical overview
Abstract
Objective: To describe the clinical recognition, pathology, and management of Richter's hernia and to review the relevant literature of the past 400 years.
Summary background data: The earliest known reported case of Richter's hernia occurred in 1598 and was described by Fabricius Hildanus. The first scientific description of this particular hernia was given by August Gottlob Richter in 1778, who presented it as "the small rupture." In 1887, Sir Frederick Treves gave an excellent overview on the topic and proposed the title "Richter's hernia." To his work-a cornerstone to modern understanding-hardly any new aspects can be added today. Since then, only occasional case reports or small series of retrospectively collected Richter's hernias have been published.
Methods: The authors draw on their experience with 18 prospectively collected cases treated in the ICRC Lopiding Hospital for War Surgery in northern Kenya between February and December 1998 and review the relevant literature of the past 400 years.
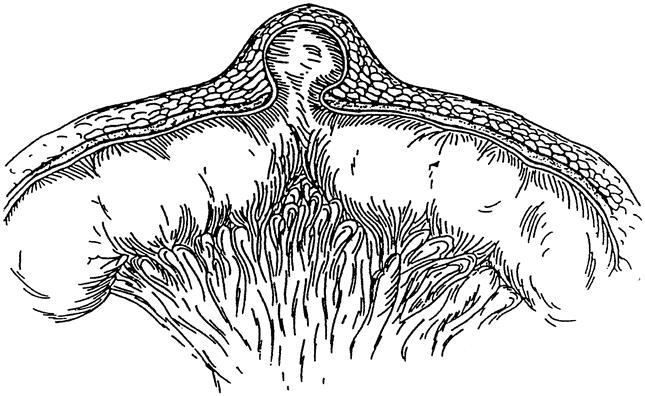
Results: The classic features of Richter's hernia were confirmed in all case studies of patients: only part of the circumference of the bowel is entrapped and strangulated in the hernial orifice. The involved segment may rapidly pass into gangrene, yet signs of intestinal obstruction are often absent. The death rate in the authors' collective was 17%.
Conclusion: Richter's hernia is a deceptive entity whose high death rate can be reduced by accurate diagnosis and early surgery. Considering the increasing incidence at laparoscope insertion sites, awareness of this special type of hernia with its misleading clinical appearance is important and of general interest.
Figures



References
-
- Tito WA, Allen WC. Richter and Littre Hernia. In: Nyhus JB, Condon RE, eds. Hernia, 3rd edition, Philadelphia: Lippincott; 1989:305–310.
-
- Giokas G, Karakousis CP. Richter hernia of the stomach. J Surg Oncol 1998; 69 (1): 51–53. - PubMed
-
- Rowe PH, Hunter-Craig C. Richter’s hernia in a direct inguinal sac in a female. J R Coll Surg Edinb 1984; 29: 264. - PubMed
-
- Newerla GJ, Connally EF. Gangrenous appendicitis in femoral hernia of Richter’s type. Am J Surg 1943; 61: 154–156.
Publication types
MeSH terms
Personal name as subject
- Actions
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
