

Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis
- PMID: 11073508
- PMCID: PMC27521
- DOI: 10.1136/bmj.321.7270.1183
Risk of gastrointestinal haemorrhage with long term use of aspirin: meta-analysis
Abstract
Objectives: To assess the incidence of gastrointestinal haemorrhage associated with long term aspirin therapy and to determine the effect of dose reduction and formulation on the incidence of such haemorrhage.
Design: Meta-analysis of 24 randomised controlled trials (almost 66 000 participants).
Intervention: Aspirin compared with placebo or no treatment, for a minimum of one year.
Main outcome measures: Incidence of gastrointestinal haemorrhage.
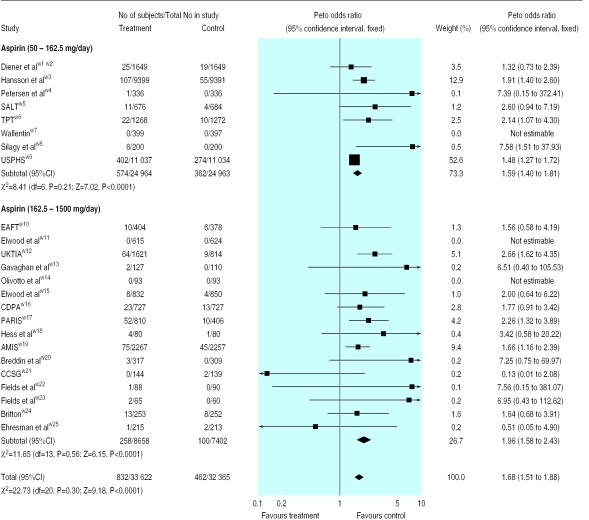
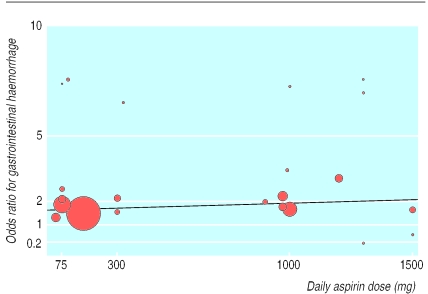
Results: Gastrointestinal haemorrhage occurred in 2.47% of patients taking aspirin compared with 1.42% taking placebo (odds ratio 1.68; 95% confidence interval 1.51 to 1.88); the number needed to harm was 106 (82 to 140) based on an average of 28 months' therapy. At doses below 163 mg/day, gastrointestinal haemorrhage occurred in 2.30% of patients taking aspirin compared with 1.45% taking placebo (1.59; 1.40 to 1.81). Meta-regression showed no relation between gastrointestinal haemorrhage and dose. For modified release formulations of aspirin the odds ratio was 1.93 (1.15 to 3.23).
Conclusions: Long term therapy with aspirin is associated with a significant increase in the incidence of gastrointestinal haemorrhage. No evidence exists that reducing the dose or using modified release formulations would reduce the incidence of gastrointestinal haemorrhage.
Figures
Comment in
-
Aspirin, like all other drugs, is a poison.BMJ. 2000 Nov 11;321(7270):1170-1. doi: 10.1136/bmj.321.7270.1170. BMJ. 2000. PMID: 11073495 Free PMC article. No abstract available.
References
-
- Bayer Pharmaceuticals. Facts about aspirin. www.wonderdrug.com/press/factsheets/aspirin_fact_sheet.pdf (accessed 28 July 2000).
-
- Zanchetti A, Hansson L. Risk of major gastrointestinal bleeding with aspirin. Lancet. 1999;353:148–150. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical