

Limited resection for early adenocarcinoma in Barrett's esophagus
- PMID: 11088068
- PMCID: PMC1421266
- DOI: 10.1097/00000658-200012000-00002
Limited resection for early adenocarcinoma in Barrett's esophagus
Abstract
Objective: To assess the extent of disease in patients with pT1 esophageal adenocarcinoma and to evaluate the feasibility and outcomes of a limited surgical approach.
Summary background data: Radical esophagectomy with systematic lymphadenectomy is widely advocated as the treatment of choice in patients with early adenocarcinoma of the distal esophagus. This approach, however, is associated with substantial complications and long-term side effects. The extent of resection necessary to achieve cure in such patients is not clear.
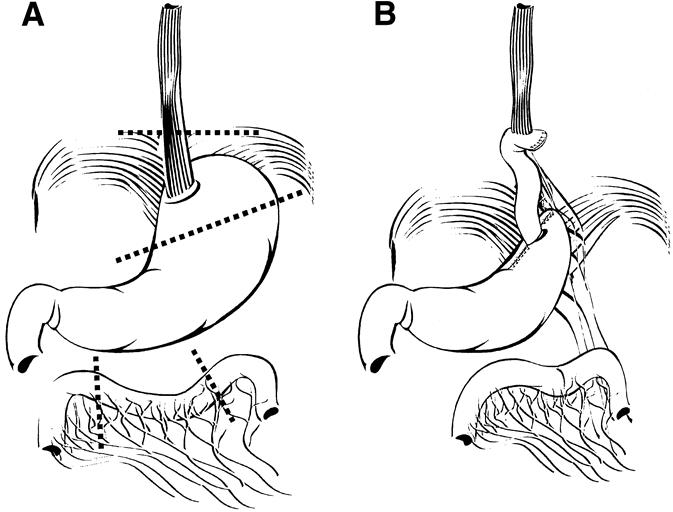
Methods: Seventy-one patients with pT1 adenocarcinoma of the distal esophagus underwent transmediastinal or transthoracic esophagectomy with two-field lymphadenectomy. Twenty-four patients with uT1N0 tumors underwent a limited resection of the distal esophagus and esophagogastric junction, regional lymphadenectomy, and reconstruction by interposition of an isoperistaltic pedicled jejunal segment. The two groups were compared for extent and multicentricity of the primary tumor and associated high-grade dysplasia, pattern of lymph node metastases, complications, deaths, and outcome of surgical treatment.
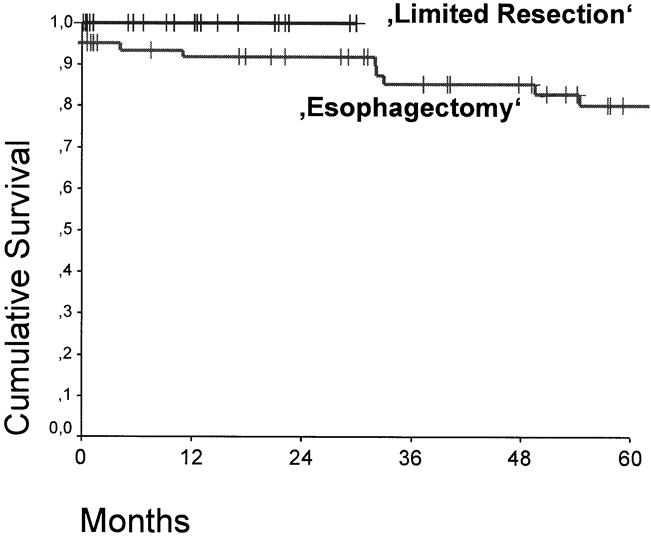
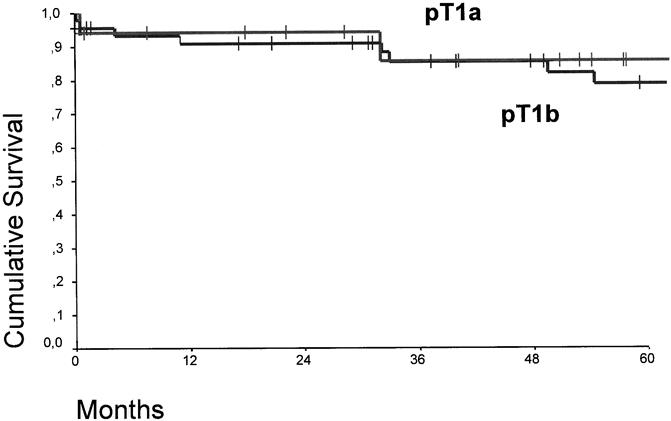
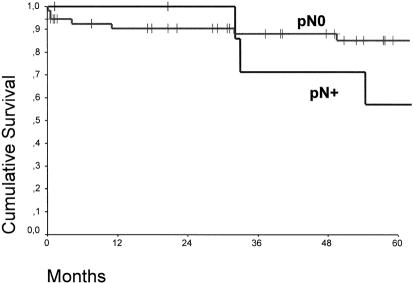
Results: Multicentric tumor growth or associated high-grade dysplasia was observed in 60.6% of the resection specimens. Complete resection of the tumor and the entire segment with intestinal metaplasia was achieved in all patients, irrespective of the surgical approach. Patients undergoing limited resection had fewer complications. Lymph node metastases or micrometastases were present in none of the 38 patients with tumors limited to the mucosa (pT1a) versus 10 of the 56 (17.9%) patients with tumors invading the submucosa (pT1b). Distant lymph node metastases occurred only in patients with more than three positive regional lymph nodes. Lymph node metastases were prognostic, but the pT1a/pT1b category and the surgical approach were not. The mean Gastrointestinal Quality of Life Index after limited resection did not differ from that of healthy controls: 20 of the 24 patients were completely asymptomatic.
Conclusions: In patients with early adenocarcinoma in the distal esophagus, resection of the distal esophagus and esophagogastric junction, with regional lymphadenectomy and jejunal interposition, is an attractive limited surgical alternative to radical esophagectomy.
Figures
References
-
- Nigro JJ, Hagen JA, DeMeester TR, et al. Prevalence and location of nodal metastases in distal esophageal adenocarcinoma confined to the wall: implications for therapy. J Thorac Cardiovasc Surg 1999; 117: 16–23. - PubMed
-
- Holscher AH, Bollschweiler E, Bumm R, et al. Prognostic factors of resected adenocarcinoma of the esophagus. Surgery 1995; 118: 845–855. - PubMed
-
- Lerut T, Coosemans W, Van Raemdonck D, et al. Surgical treatment of Barrett’s carcinoma. Correlations between morphologic findings and prognosis. J Thorac Cardiovasc Surg 1994; 107: 1059–1065. - PubMed
-
- Hagen JA, Peters JH, DeMeester TR. Superiority of extended en bloc esophagogastrectomy for carcinoma of the lower esophagus and cardia. J Thorac Cardiovasc Surg 1993; 106: 850–859. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
