

Hepatic resection for colorectal liver metastases: A cost-effectiveness analysis
- PMID: 11088071
- PMCID: PMC1421269
- DOI: 10.1097/00000658-200012000-00005
Hepatic resection for colorectal liver metastases: A cost-effectiveness analysis
Abstract
Objective: To analyze the cost-effectiveness of resection for liver metastases compared with standard nonsurgical cytotoxic treatment.
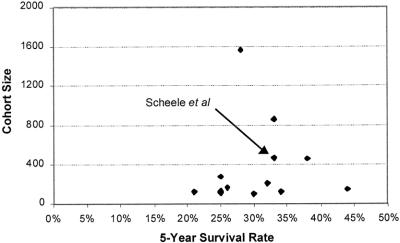
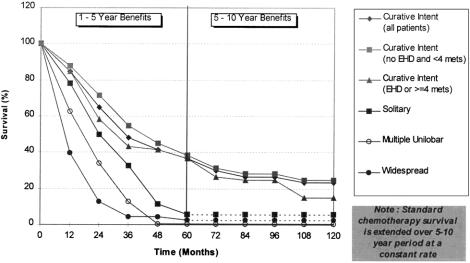
Summary background data: The efficacy of hepatic resection for metastases from colorectal cancer has been debated, despite reported 5-year survival rates of 20% to 40%. Resection is confined to specialized centers and is not widely available, perhaps because of lack of appropriate expertise, resources, or awareness of its efficacy. The cost-effectiveness of resection is important from the perspective of managed care in the United States and for the commissioning of health services in the United Kingdom.
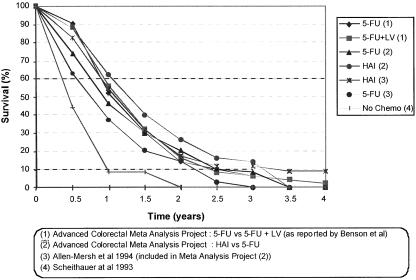
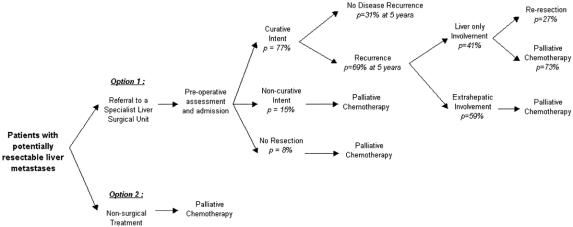
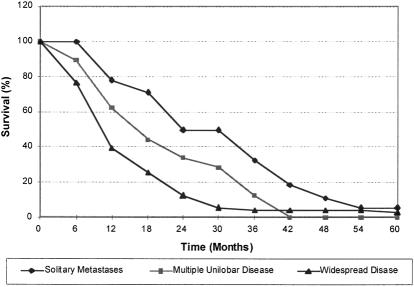
Methods: A simple decision-based model was developed to evaluate the marginal costs and health benefits of hepatic resection. Estimates of resectability for liver metastases were taken from UK-reported case series data. The results of 100 hepatic resections conducted in Sheffield from 1997 to 1999 were used for the cost calculation of liver resection. Survival data from published series of resections were compiled to estimate the incremental cost per life-year gained (LYG) because of the short period of follow-up in the Sheffield series.
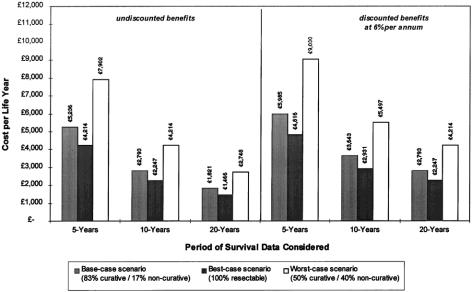
Results: Hepatic resection for colorectal liver metastases provides an estimated marginal benefit of 1.6 life-years (undiscounted) at a marginal cost of 6,742 pound sterling++. If 17% of patients have only palliative resections, the overall cost per LYG is approximately 5,236 pound sterling (5,985 pound sterling with discounted benefits). If potential benefits are extended to include 20-year survival rates, these figures fall to approximately 1,821 pound sterling (2,793 pound sterling with discounted benefits). Further univariate sensitivity analysis of key model parameters showed the cost per LYG to be consistently less than 15,000 pound sterling.
Conclusion: In this model, hepatic resection appears highly cost-effective compared with nonsurgical treatments for colorectal-related liver metastases.
Figures
References
-
- Office for National Statistics. Cancer Statistics: Registrations MB1 no. 25. London: HMSO; 1992.
-
- Colorectal Cancer in Trent, 1992–94. Trent Cancer Registry; 1998.
-
- NHS Center for Reviews and Dissemination. Effective Health Care: The Management of Colorectal Cancer, Vol. 3, No. 6. York: University of York; 1997.
-
- NHS Executive. Guidance on Commissioning Cancer Services: Improving Outcomes in Colorectal Cancer: The Research Evidence. London: Department of Health; 1997.
-
- Millikan KW, Staren ED, Doolas A. Invasive therapy of metastatic colorectal cancer to the liver. Surg Clin North Am 1997; 77: 27–48. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
