

Extracorporeal membrane oxygenation for severe acute respiratory failure
- PMID: 11094500
- PMCID: PMC137254
- DOI: 10.1186/cc689
Extracorporeal membrane oxygenation for severe acute respiratory failure
Abstract
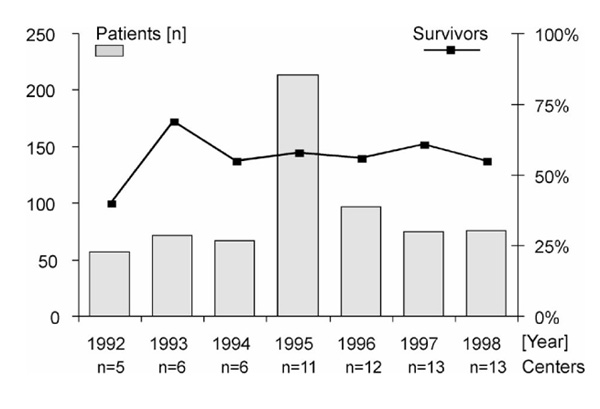
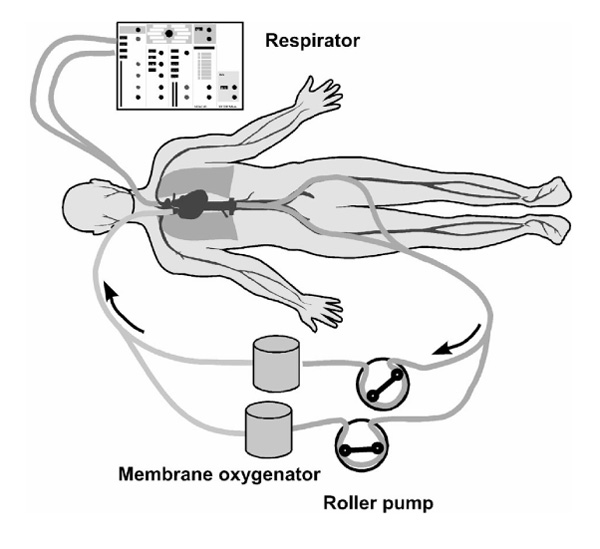
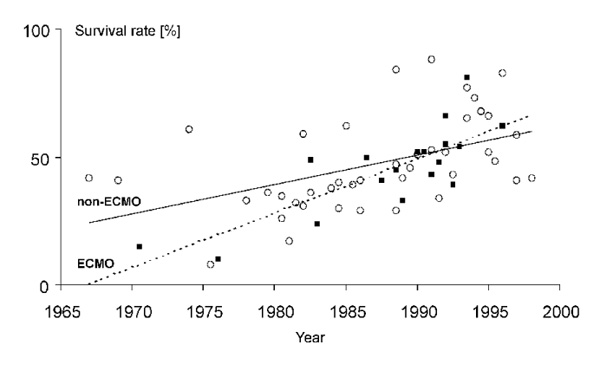
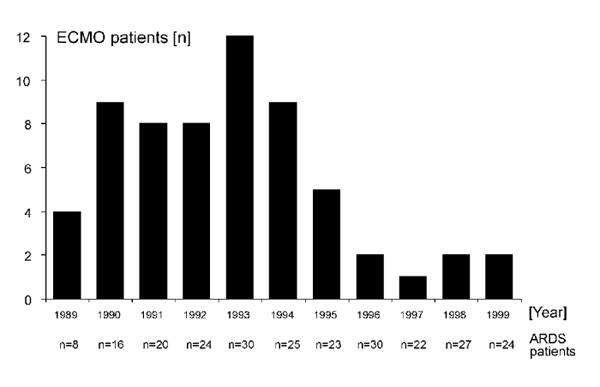
Extracorporeal membrane oxygenation (ECMO) is a technique for providing life support, in case the natural lungs are failing and are not able to maintain a sufficient oxygenation of the body's organ systems. ECMO technique was an adaptation of conventional cardiopulmonary bypass techniques and introduced into treatment of severe acute respiratory distress syndrome (ARDS) in the 1970s. The initial reports of the use of ECMO in ARDS patients were quite enthusiastic, however, in the following years it became clear that ECMO was only of benefit in newborns with acute respiratory failure. In neonates treated with ECMO, survival rates of 80% could be achieved. In adult patients with ARDS, two large randomized controlled trials (RCTs) published in 1979 and 1994 failed to show an advantage of ECMO over conventional treatment; survival rates were only 10% and 33%, respectively, in the ECMO groups. Since then, ECMO technology as well as conventional treatment of adult ARDS have undergone further improvements. In conventional treatment lung-protective ventilation strategies were introduced and ECMO was made safer by applying heparin-coated equipment, membranes and tubings. Many ECMO centres now use these advanced ECMO technology and report survival rates in excess of 50% in uncontrolled data collections. The question, however, of whether the improved ECMO can really challenge the advanced conventional treatment of adult ARDS is unanswered and will need evaluation by a future RCT.
Figures
References
-
- Luhr OR, Antonsen K, Karlsson M, et al. Incidence and mortality after acute respiratory failure and acute respiratory distress syndrome in Sweden, Denmark, and Iceland. Am J Respir Crit Care Med. 1999;159:1849–1861. - PubMed
-
- Lewandowski K, Metz J, Deutschmann C, et al. Incidence, severity, and mortality of acute respiratory failure in Berlin, Germany. Am J Respir Crit Care Med. 1995;151:1121–1125. - PubMed
-
- Kanazawa M. Acute lung injury: clinical concept and experimental approaches to pathogenesis. Keio J Med. 1996;45:131–139. - PubMed
-
- Luce JM. Acute lung injury and the acute respiratory distress syndrome. Crit Care Med. 1998;26:369–376. - PubMed
-
- Webster NR, Cohen AT, Nunn JF. Adult respiratory distress syndrome: how many cases in the UK? Anaesthesia. 1988;43:923–926. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
