

Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation
- PMID: 11094507
- PMCID: PMC137257
- DOI: 10.1186/cc710
Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation
Abstract
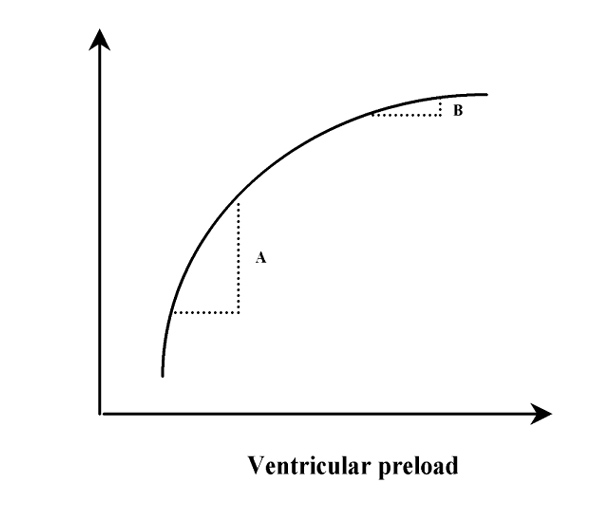
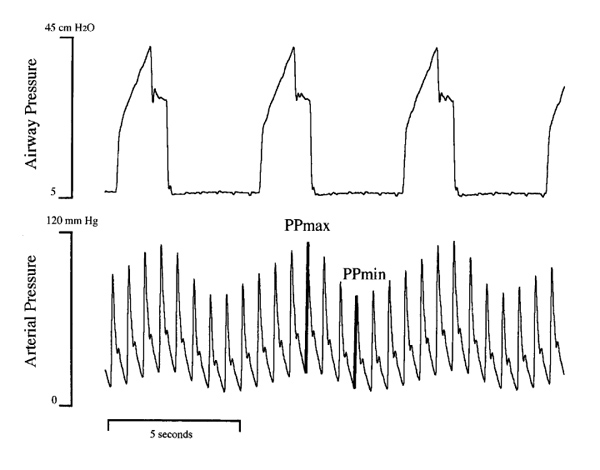
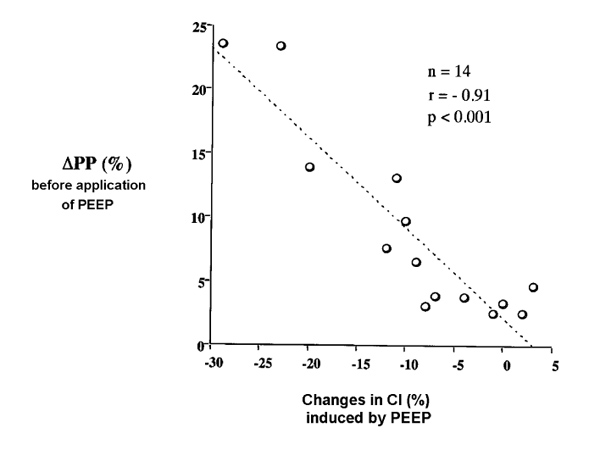
According to the Frank-Starling relationship, a patient is a 'responder' to volume expansion only if both ventricles are preload dependent. Mechanical ventilation induces cyclic changes in left ventricular (LV) stroke volume, which are mainly related to the expiratory decrease in LV preload due to the inspiratory decrease in right ventricular (RV) filling and ejection. In the present review, we detail the mechanisms by which mechanical ventilation should result in greater cyclic changes in LV stroke volume when both ventricles are 'preload dependent'. We also address recent clinical data demonstrating that respiratory changes in arterial pulse (or systolic) pressure and in Doppler aortic velocity (as surrogates of respiratory changes in LV stroke volume) can be used to detect biventricular preload dependence, and hence fluid responsiveness in critically ill patients.
Figures




References
-
- Braunwald E, Sonnenblick EH, Ross J. Mechanisms of cardiac contraction and relaxation. Heart Disease. Edited by Braunwald E. Philadelphia: WB Saunders company; 1988. pp. 383–425.
-
- Nixon JV, Murray RG, Leonard PD, Mitchell JH, Blomqvist CG. Effect of large variations in preload on left ventricular performance characteristics in normal subjects. Circulation. 1982;65:698–703. - PubMed
-
- Calvin JE, Driedger AA, Sibbald WJ. The hemodynamic effect of rapid fluid infusion in critically ill patients. Surgery. 1981;90:61–76. - PubMed
-
- Reuse C, Vincent JL, Pinsky MR. Measurements of right ventricular volumes during fluid challenge. Chest. 1990;98:1450–1454. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
