

Transplanted fetal striatum in Huntington's disease: phenotypic development and lack of pathology
- PMID: 11106399
- PMCID: PMC17669
- DOI: 10.1073/pnas.97.25.13877
Transplanted fetal striatum in Huntington's disease: phenotypic development and lack of pathology
Abstract
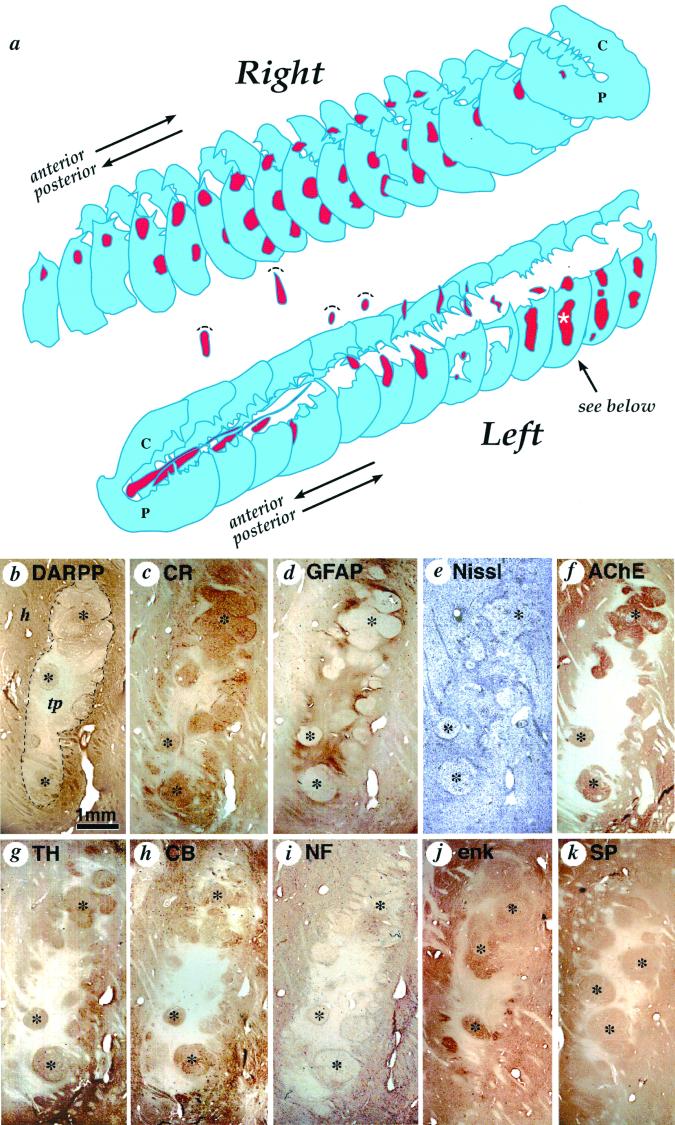
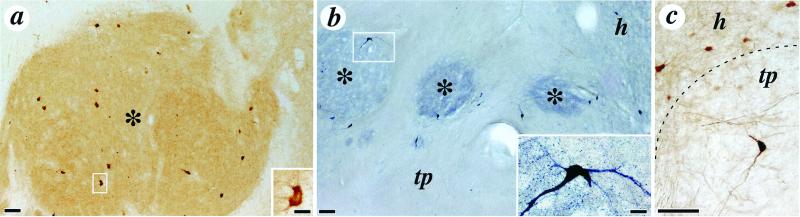
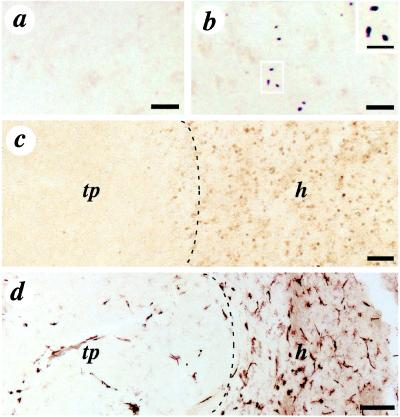
Neural and stem cell transplantation is emerging as a potential treatment for neurodegenerative diseases. Transplantation of specific committed neuroblasts (fetal neurons) to the adult brain provides such scientific exploration of these new potential therapies. Huntington's disease (HD) is a fatal, incurable autosomal dominant (CAG repeat expansion of huntingtin protein) neurodegenerative disorder with primary neuronal pathology within the caudate-putamen (striatum). In a clinical trial of human fetal striatal tissue transplantation, one patient died 18 months after transplantation from cardiovascular disease, and postmortem histological analysis demonstrated surviving transplanted cells with typical morphology of the developing striatum. Selective markers of both striatal projection and interneurons such as dopamine and c-AMP-related phosphoprotein, calretinin, acetylcholinesterase, choline acetyltransferase, tyrosine hydroxylase, calbindin, enkephalin, and substance P showed positive transplant regions clearly innervated by host tyrosine hydroxylase fibers. There was no histological evidence of immune rejection including microglia and macrophages. Notably, neuronal protein aggregates of mutated huntingtin, which is typical HD neuropathology, were not found within the transplanted fetal tissue. Thus, although there is a genetically predetermined process causing neuronal death within the HD striatum, implanted fetal neural cells lacking the mutant HD gene may be able to replace damaged host neurons and reconstitute damaged neuronal connections. This study demonstrates that grafts derived from human fetal striatal tissue can survive, develop, and are unaffected by the disease process, at least for 18 months, after transplantation into a patient with HD.
Figures
Comment in
-
Novel therapies in the search for a cure for Huntington's disease.Proc Natl Acad Sci U S A. 2001 Jan 2;98(1):3-4. doi: 10.1073/pnas.98.1.3. Proc Natl Acad Sci U S A. 2001. PMID: 11136240 Free PMC article. No abstract available.
References
-
- Dunnett S B. Neuropathol Appl Neurobiol. 1999;25:351–362. - PubMed
-
- Shihabuddin L S, Palmer T D, Gage F H. Mol Med Today. 1999;5:474–480. - PubMed
-
- The Huntington's Disease Collaborative Research Group. Cell. 1993;72:971–983. - PubMed
-
- DiFiglia M, Sapp E, Chase K O, Davies S W, Bates G P, Vonsattel J P, Aronin N. Science. 1997;277:1990–1993. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
