

High-b-value diffusion-weighted MR imaging of suspected brain infarction
- PMID: 11110533
- PMCID: PMC7974302
High-b-value diffusion-weighted MR imaging of suspected brain infarction
Abstract
Background and purpose: Recent technological advances in MR instrumentation allow acquisition of whole-brain diffusion-weighted MR scans to be obtained with b values greater than 1,000. Our purpose was to determine whether high-b-value diffusion-weighted MR imaging improved contrast and detection of signal changes in acute and chronic brain infarction.
Methods: We prospectively evaluated the MR scans of 30 subjects with a history of possible brain infarction on a 1.5-T MR imager with 40 mT/meter gradients (slew rate 150 T/m/s) by use of the following single-shot echo-planar diffusion-weighted MR sequences: 1) 7,999/ 71.4/1 (TR/TE/excitations, b = 1,000; 2) 999/ 88.1/3, b = 2,500; and 3) 7,999/ 92.1/4, b = 3,000. Diffusion-weighted MR imaging was performed in three orthogonal directions during all sequences. All subjects were scanned with fast fluid-attenuated inversion recovery (FLAIR) (10,006/145/2,200/1 [TR/TE/TI/excitations]) and fast spin-echo T2-weighted (3,650/95/3 [TR/TE/excitations], echo train length, 8). The diagnosis of brain infarction was established by clinical criteria.
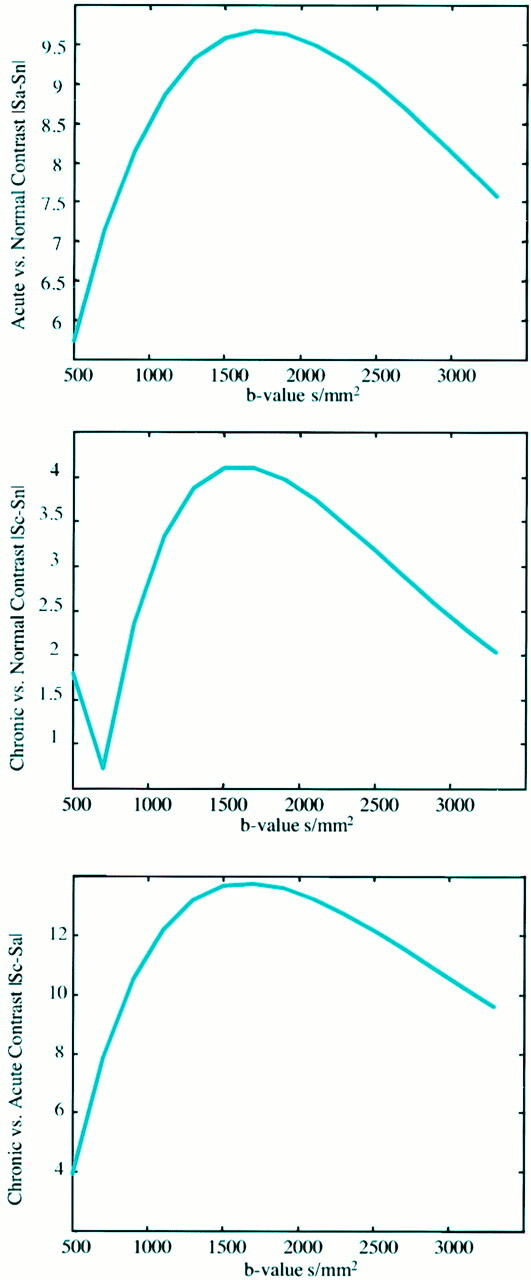
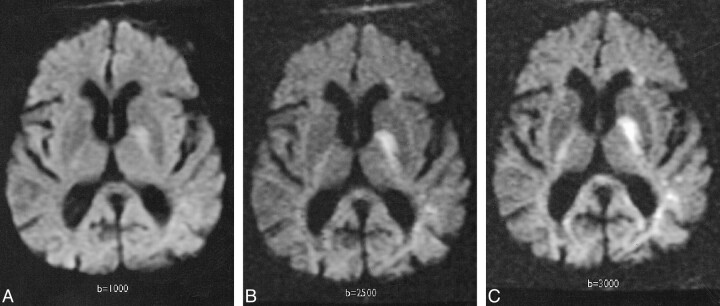
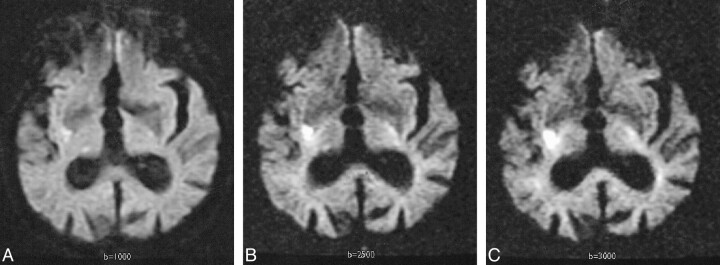
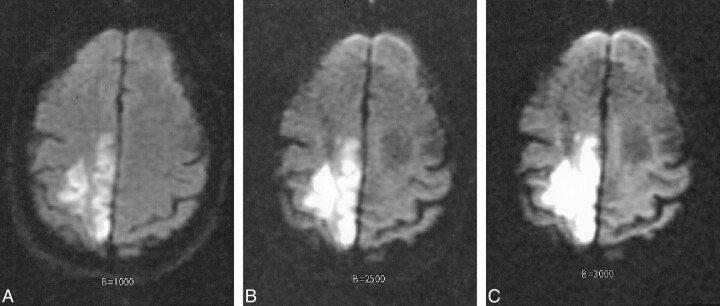
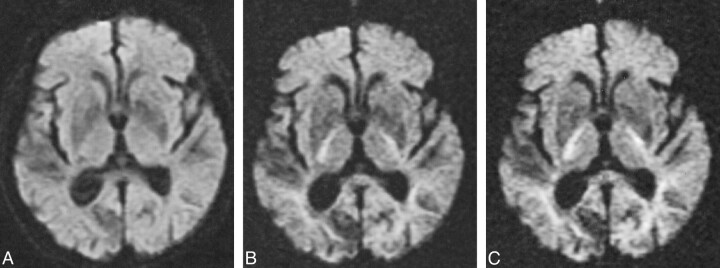
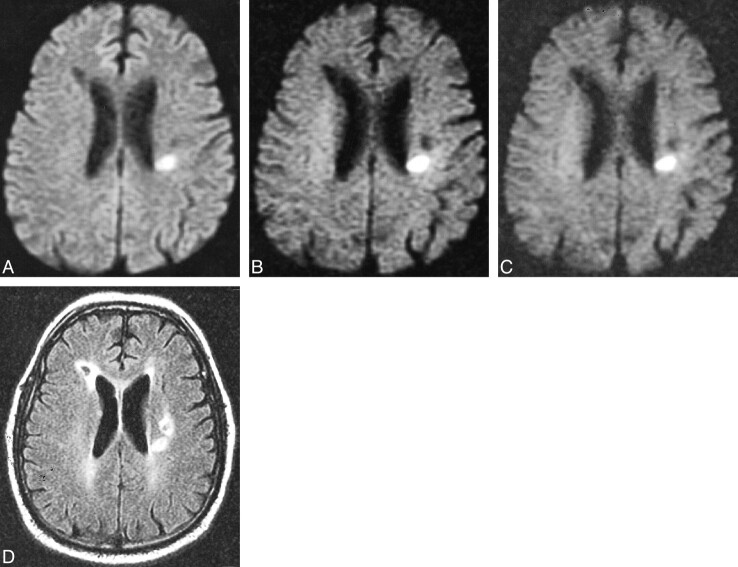
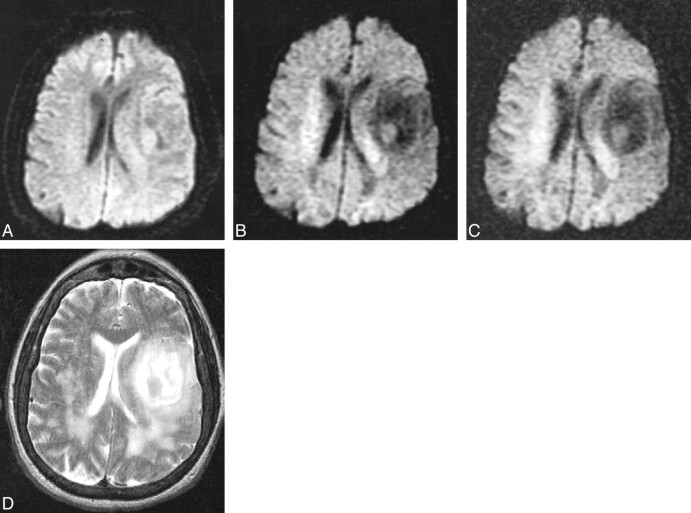
Results: Twenty women and 10 men with a mean age of 67.7 years were enrolled in the study. One subject was excluded owing to poor image quality. Twelve of 29 subjects had a clinical diagnosis of acute infarction. All 12 had lesions that were hyperintense on diffusion-weighted images at all three b values; five were cortical and seven subcortical. There was increased contrast of all lesions on high-b-value scans (b = 2,500 and 3,000). Lesions that were hypointense on diffusion-weighted images were identified and evaluated at the three different b values. At b = 1,000, there were 19 hypointense lesions, whereas at b = 2,500 and 3,000 there were 48 and 55 lesions, respectively. On FLAIR and T2-weighted images, these low-signal lesions were predominantly chronic, subcortical, ischemic lesions and lacunar infarcts, but four chronic cortical infarcts, one porencephalic cyst, and one primary brain tumor were also found. Low-signal lesions were also noted to have increased contrast on high-b-value diffusion-weighted scans.
Conclusion: High-b-value diffusion-weighted MR imaging (b = 2,500 or b = 3,000) had no impact on diagnosis of acute infarction. High-b-value diffusion-weighted MR imaging (b = 2,500) combined with diffusion-weighted MR imaging at b = 1,000 improves tissue characterization by increasing the spectrum of observed imaging abnormalities in patients with suspected brain infarction.
Figures
Comment in
-
Diffusing into the future.AJNR Am J Neuroradiol. 2000 Nov-Dec;21(10):1780-2. AJNR Am J Neuroradiol. 2000. PMID: 11110526 Free PMC article. No abstract available.
References
-
- Benveniste H, Johnson GA. Mechanisms of ischemia-induced changes in brain water diffusion coefficient studied by brain MRI and brain microdialysis. Stroke 1992;23:746-754
-
- Baker LL, Kucharcyzk J, Sevick RJ, Mintorovich J, Moseley M. Recent advances in MR imaging/spectroscopy of cerebral ischemia. AJR Am J Roentgenol 1991; 156:1133-1143 - PubMed
-
- Sevick RJ, Kanda F, Mintorovich J, et al. Cytotoxic brain edema: assessment with diffusion-weighted MR imaging. Radiology 1992;185:687-690 - PubMed
-
- Mintorovich J, Baker LL, Yang GY, et al. Diffusion weighted hyperintensity in early cerebral ischemia: correlation with brain water content and ATPase activity. Proc Soc Magn Reson 1991;10:329
MeSH terms
LinkOut - more resources
Full Text Sources