

Randomised controlled trial of dual blockade of renin-angiotensin system in patients with hypertension, microalbuminuria, and non-insulin dependent diabetes: the candesartan and lisinopril microalbuminuria (CALM) study
- PMID: 11110735
- PMCID: PMC27545
- DOI: 10.1136/bmj.321.7274.1440
Randomised controlled trial of dual blockade of renin-angiotensin system in patients with hypertension, microalbuminuria, and non-insulin dependent diabetes: the candesartan and lisinopril microalbuminuria (CALM) study
Abstract
Objectives: To assess and compare the effects of candesartan or lisinopril, or both, on blood pressure and urinary albumin excretion in patients with microalbuminuria, hypertension, and type 2 diabetes.
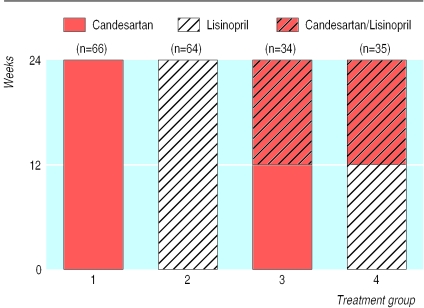
Design: Prospective, randomised, parallel group, double blind study with four week placebo run in period and 12 weeks' monotherapy with candesartan or lisinopril followed by 12 weeks' monotherapy or combination treatment.
Setting: Tertiary hospitals and primary care centres in four countries (37 centres).
Participants: 199 patients aged 30-75 years.
Interventions: Candesartan 16 mg once daily, lisinopril 20 mg once daily.
Main outcome measures: Blood pressure and urinary albumin:creatinine ratio.
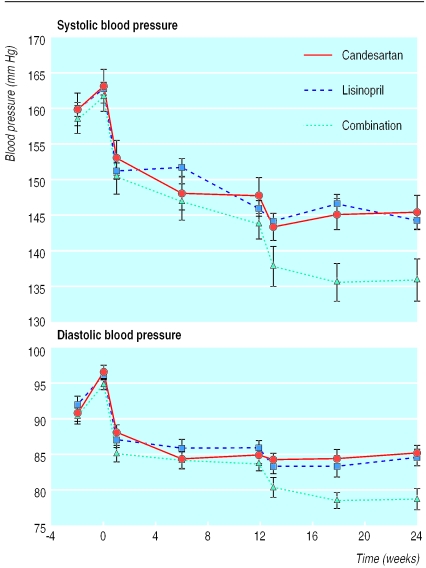
Results: At 12 weeks mean (95% confidence interval) reductions in diastolic blood pressure were 9.5 mm Hg (7.7 mm Hg to 11.2 mm Hg, P<0.001) and 9.7 mm Hg (7.9 mm Hg to 11.5 mm Hg, P<0.001), respectively, and in urinary albumin:creatinine ratio were 30% (15% to 42%, P<0.001) and 46% (35% to 56%, P<0.001) for candesartan and lisinopril, respectively. At 24 weeks the mean reduction in diastolic blood pressure with combination treatment (16.3 mm Hg, 13.6 mm Hg to 18.9 mm Hg, P<0. 001) was significantly greater than that with candesartan (10.4 mm Hg, 7.7 mm Hg to 13.1 mm Hg, P<0.001) or lisinopril (mean 10.7 mm Hg, 8.0 mm Hg to 13.5 mm Hg, P<0.001). Furthermore, the reduction in urinary albumin:creatinine ratio with combination treatment (50%, 36% to 61%, P<0.001) was greater than with candesartan (24%, 0% to 43%, P=0.05) and lisinopril (39%, 20% to 54%, P<0.001). All treatments were generally well tolerated.
Conclusion: Candesartan 16 mg once daily is as effective as lisinopril 20 mg once daily in reducing blood pressure and microalbuminuria in hypertensive patients with type 2 diabetes. Combination treatment is well tolerated and more effective in reducing blood pressure.
Figures
Comment in
- ACP J Club. 2001 Jul-Aug;135(1):9
-
Dual blockade of renin-angiotensin system. Data do not support claimed benefit of combination over single treatment.BMJ. 2001 May 12;322(7295):1183. BMJ. 2001. PMID: 11379586 Free PMC article. No abstract available.
References
-
- Cooper ME. Pathogenesis, prevention and treatment of diabetic nephropathy. Lancet. 1998;352:213–219. - PubMed
-
- Mogensen CE, Keane WF, Bennett PH, Jerums G, Parving HH, Passa P, et al. Prevention of diabetic renal disease with special reference to microalbuminuria. Lancet. 1995;346:1080–1084. - PubMed
-
- Azizi M, Chatellier G, Guyene TT, Murietageoffroy D, Menard J. Additive effects of combined angiotensin-converting enzyme inhibition and angiotensin II antagonism on blood pressure and renin release in sodium-depleted normotensives. Circulation. 1995;92:825–834. - PubMed
-
- Hollenberg NK, Fisher NDL, Price DA. Pathways for angiotensin II generation in intact human tissue—evidence from comparative pharmacological interruption of the renin system. Hypertension. 1998;32:387–392. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical