

Right ventricular diastolic dysfunction in patients with anticardiolipin antibodies and antiphospholipid syndrome
- PMID: 11114281
- PMCID: PMC1753369
- DOI: 10.1136/ard.60.1.43
Right ventricular diastolic dysfunction in patients with anticardiolipin antibodies and antiphospholipid syndrome
Abstract
Objective: To evaluate the prevalence of diastolic dysfunction in patients with anticardiolipin antibodies (aCL) and to examine whether the antiphospholipid syndrome (APS) is associated with diastolic dysfunction independently of valvular abnormalities and systolic dysfunction.
Methods: Pulsed, continuous, colour Doppler echocardiography was performed in 179 subjects, of whom 15 were excluded from the analysis because of systolic dysfunction or severe valvular disease. The remaining 164 subjects included 29 patients with primary APS, 26 patients with secondary APS (APS in the presence of systemic lupus erythematosus (SLE)), and 30 patients with SLE and aCL but without APS; 43 patients with SLE without aCL and 36 normal volunteers served as control groups.
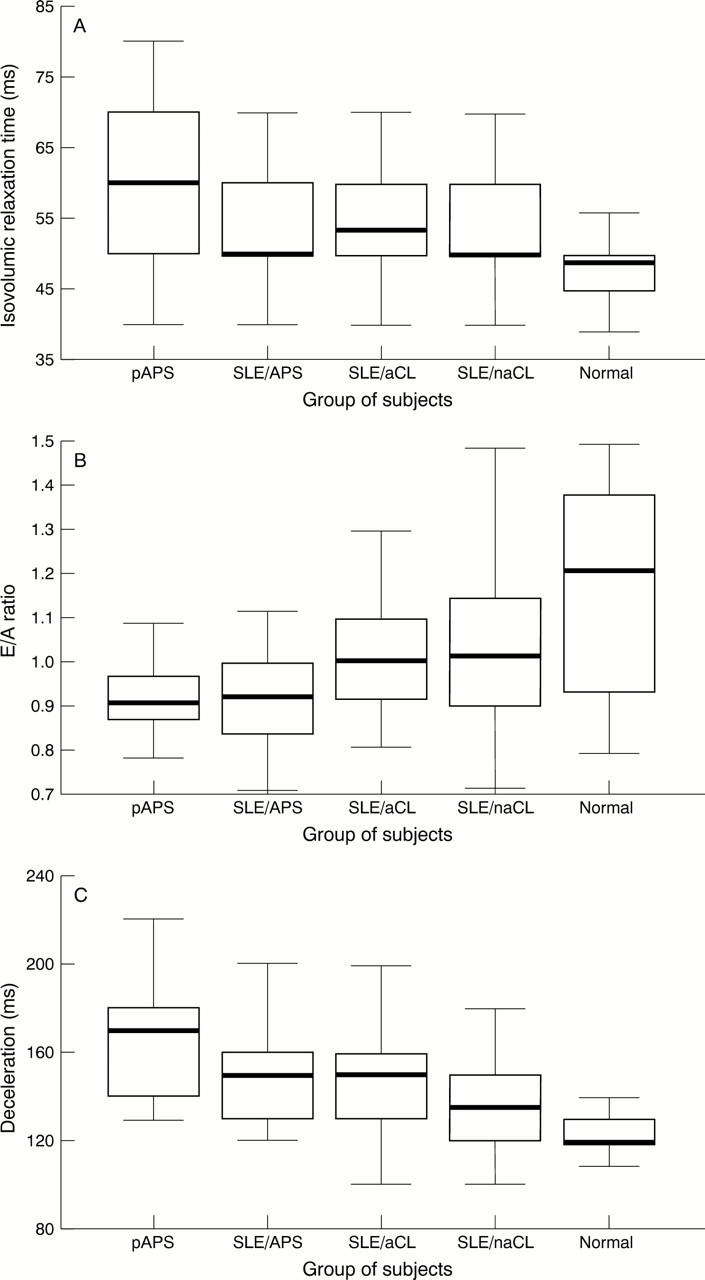
Results: The groups compared differed significantly in all measures of right ventricular function. There was a gradation of increasing diastolic function impairment as manifested by prolonged deceleration time (DT) and isovolumic relaxation time (IVRT) across the groups of patients with SLE without aCL, SLE with aCL, secondary APS, and primary APS. Differences in left ventricular diastolic function measures were less prominent. In regression analysis, DT increased by 19.6 ms (p=0.002) in the presence of primary APS and by 20.1 ms (p=0.038) in the presence of pulmonary hypertension. The titre of IgG aCL was the strongest predictor of a prolonged IVRT.
Conclusion: Diastolic dysfunction, in particular of the right ventricle-that is, independent of valvular disease and systolic dysfunction, is a prominent feature of APS and may be related to the pathogenesis of the syndrome.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
