

Double blind, randomised, placebo controlled study of a platelet activating factor antagonist, lexipafant, in the treatment and prevention of organ failure in predicted severe acute pancreatitis
- PMID: 11115824
- PMCID: PMC1728186
- DOI: 10.1136/gut.48.1.62
Double blind, randomised, placebo controlled study of a platelet activating factor antagonist, lexipafant, in the treatment and prevention of organ failure in predicted severe acute pancreatitis
Abstract
Background: Platelet activating factor (PAF) is believed to amplify the activity of key mediators of the systemic inflammatory response syndrome (SIRS) in acute pancreatitis, resulting in multiorgan dysfunction syndrome. We tested the hypothesis that a potent PAF antagonist, lexipafant, could dampen SIRS and reduce organ failure in severe acute pancreatitis.
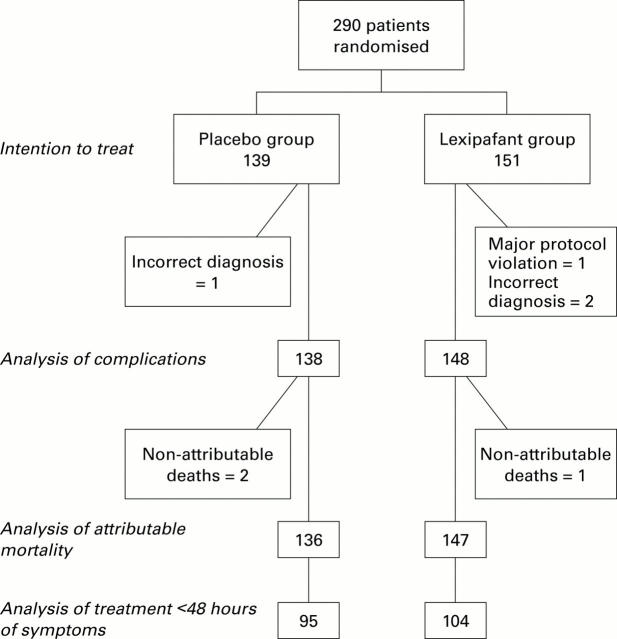
Methods: We conducted a randomised, double blind, placebo controlled, multicentre trial of lexipafant (100 mg/24 hours intravenously for seven days commenced within 72 hours of the onset of symptoms) involving 290 patients with an APACHE II score >6. Power calculations assumed that complications would be reduced from 40% to 24%. Secondary end points studied included severity of organ failure, markers of the inflammatory response, and mortality rate.
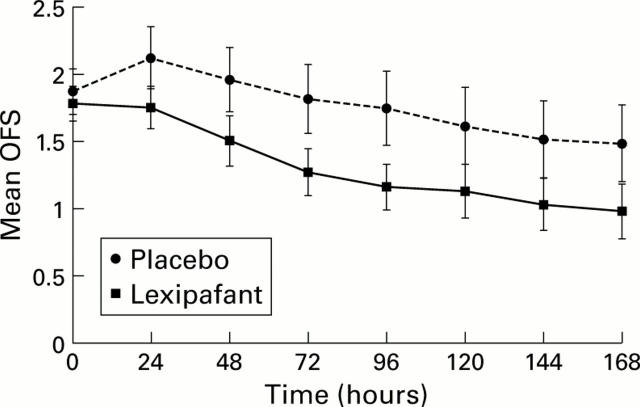
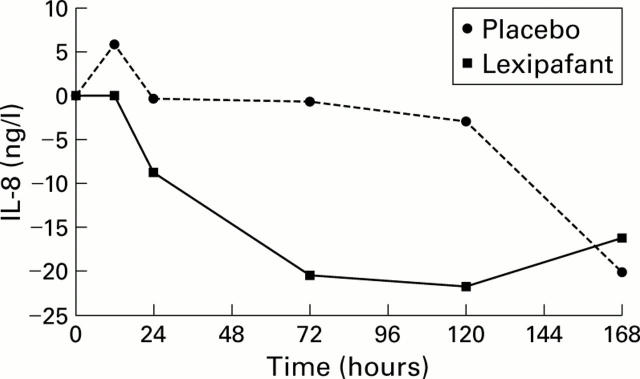
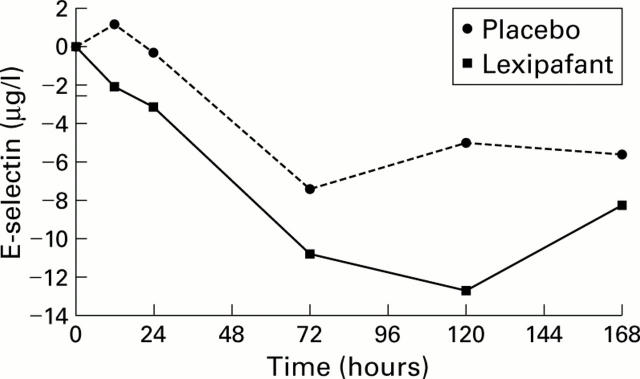
Findings: Overall, 80/138 (58%) patients in the placebo group and 85/148 (57%) in the lexipafant group developed one or more organ failures. The primary hypothesis was invalidated by the unexpected finding that 44% of patients had organ failure on entry into the study; only 39 (14%) developed new organ failure. Organ failure scores were reduced in the lexipafant group only on day 3: median change -1 (range -4 to +8) versus 0 (-4 to +10) in the placebo group (p=0.04). Systemic sepsis affected fewer patients in the lexipafant group (13/138 v 4/148; p=0.023). Local complications occurred in 41/138 (30%) patients in the placebo group and in 30/148 (20%) in the lexipafant group (20%; p=0.065); pseudocysts developed in 19 (14%) and eight (5%) patients, respectively (p=0.025). Deaths attributable to acute pancreatitis were not significantly different. Interleukin 8, a marker of neutrophil activation, and E-selectin, a marker of endothelial damage, decreased more rapidly in the lexipafant group (both p<0.05); however, absolute values were not different between the two groups.
Interpretation: The high incidence of organ failure within 72 hours of the onset of symptoms undermined the primary hypothesis, and power calculations for future studies in severe acute pancreatitis will need to allow for this. Lexipafant had no effect on new organ failure during treatment. This adequately powered study has shown that antagonism of PAF activity on its own is not sufficient to ameliorate SIRS in severe acute pancreatitis
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical