

Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials
- PMID: 11118174
- PMCID: PMC27550
- DOI: 10.1136/bmj.321.7275.1493
Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials
Abstract
Objectives: To obtain reliable estimates of the effects of neuraxial blockade with epidural or spinal anaesthesia on postoperative morbidity and mortality.
Design: Systematic review of all trials with randomisation to intraoperative neuraxial blockade or not.
Studies: 141 trials including 9559 patients for which data were available before 1 January 1997. Trials were eligible irrespective of their primary aims, concomitant use of general anaesthesia, publication status, or language. Trials were identified by extensive search methods, and substantial amounts of data were obtained or confirmed by correspondence with trialists.
Main outcome measures: All cause mortality, deep vein thrombosis, pulmonary embolism, myocardial infarction, transfusion requirements, pneumonia, other infections, respiratory depression, and renal failure.
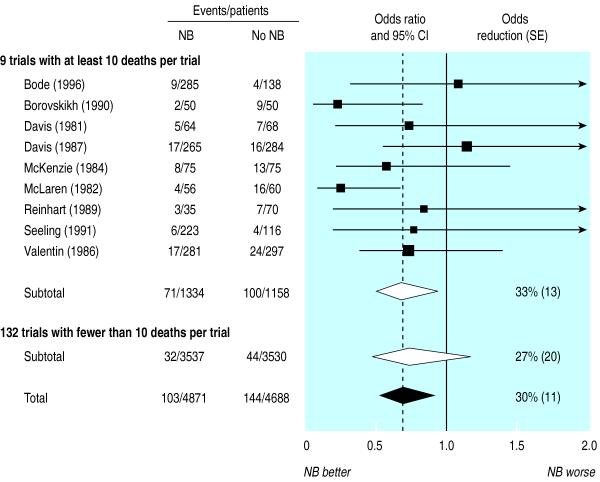
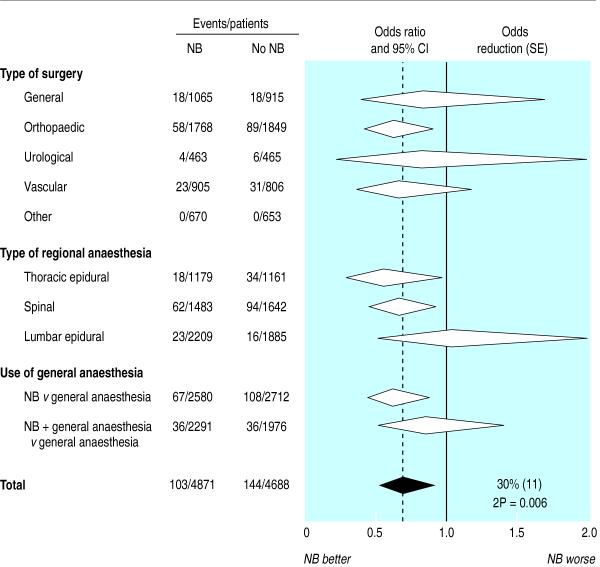
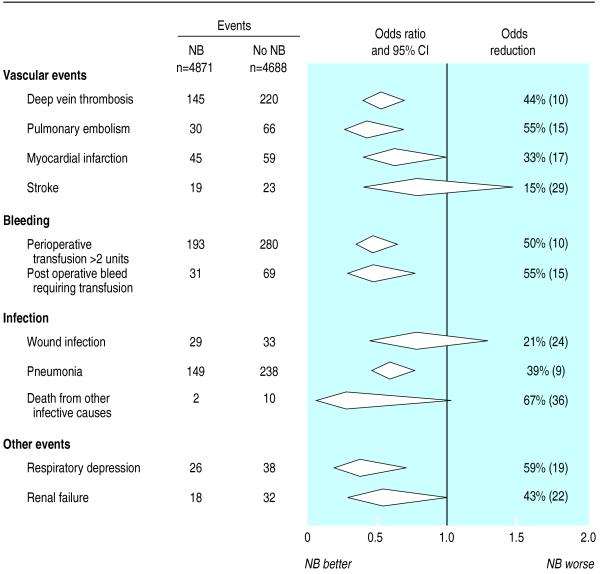
Results: Overall mortality was reduced by about a third in patients allocated to neuraxial blockade (103 deaths/4871 patients versus 144/4688 patients, odds ratio=0.70, 95% confidence interval 0.54 to 0.90, P=0. 006). Neuraxial blockade reduced the odds of deep vein thrombosis by 44%, pulmonary embolism by 55%, transfusion requirements by 50%, pneumonia by 39%, and respiratory depression by 59% (all P<0.001). There were also reductions in myocardial infarction and renal failure. Although there was limited power to assess subgroup effects, the proportional reductions in mortality did not clearly differ by surgical group, type of blockade (epidural or spinal), or in those trials in which neuraxial blockade was combined with general anaesthesia compared with trials in which neuraxial blockade was used alone.
Conclusions: Neuraxial blockade reduces postoperative mortality and other serious complications. The size of some of these benefits remains uncertain, and further research is required to determine whether these effects are due solely to benefits of neuraxial blockade or partly to avoidance of general anaesthesia. Nevertheless, these findings support more widespread use of neuraxial blockade.
Figures
Comment in
- ACP J Club. 20001 Jul-Aug;135(1):1
-
Reduction of postoperative mortality and morbidity. Research into modern anaesthesia techniques and perioperative medicine is needed.BMJ. 2001 May 12;322(7295):1182-3. BMJ. 2001. PMID: 11379584 No abstract available.
-
Reduction of postoperative mortality and morbidity. Little information was given on inclusion criteria.BMJ. 2001 May 12;322(7295):1182; author reply 1182-3. BMJ. 2001. PMID: 11379585 Free PMC article. No abstract available.
References
-
- Cousins M, Bridenbaugh P, editors. Neural blockade in clinical anesthesia and management of pain. 2nd ed. Philadelphia: J B Lippincott; 1988.
-
- Kehlet H. Modification of responses to surgery by neural blockade: clinical implications. In: Cousins M, Bridenbaugh P, editors. Neural blockade in clinical anesthesia and management of pain. 2nd ed. Philadelphia: J B Lippincott; 1988. pp. 145–188.
-
- Dickersin K, Larson K. Establishing and maintaining an international register of RCTs. Oxford: Cochrane Collaboration; 1995.
-
- Greenland S. Quality scores are useless and potentially misleading. Am J Epidemiol. 1994;140:300–301.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical