

Cue-dose training with monetary reinforcement: pilot study of an antiretroviral adherence intervention
- PMID: 11119180
- PMCID: PMC1495713
- DOI: 10.1046/j.1525-1497.2000.00127.x
Cue-dose training with monetary reinforcement: pilot study of an antiretroviral adherence intervention
Abstract
Objective: To assess the feasibility and efficacy of two interventions for improving adherence to antiretroviral therapy regimens in HIV-infected subjects compared with a control intervention.
Design: Randomized, controlled, pilot study.
Setting: Department of Veterans Affairs HIV clinic and community-based HIV clinical trials site.
Participants: Fifty-five HIV-infected subjects on stable antiretroviral therapy regimens. Subjects were predominantly male (89%) and African American (69%), and had histories of heroin or cocaine use (80%).
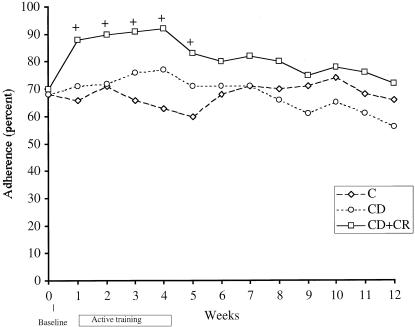
Interventions: Four weekly sessions of either nondirective inquiries about adherence (control group, C), cue-dose training, which consisted of the use of personalized cues for remembering particular dose times, and feedback about medication taking using Medication Event Monitoring System (MEMS) pill bottle caps, which record time of bottle opening (CD group), or cue-dose training combined with cash reinforcement for correctly timed bottle opening (CD+CR).
Measurements: Opening of the pill bottle within 2 hours before or after a predetermined time was measured by MEMS.
Results: Adherence to the medication as documented by MEMS was significantly enhanced during the 4-week training period in the CD+CR group, but not in the CD group, compared with the control group. Improvement was also seen in adherence to antiretroviral drugs that were not the object of training and reinforcement. Eight weeks after training and reinforcement were discontinued, adherence in the cash-reinforced group returned to near-baseline levels.
Conclusions: Cue-dose training with cash reinforcement led to transient improvement in adherence to antiretroviral therapy in a population including mostly African Americans and subjects with histories of drug abuse. However, we were not able to detect any sustained improvement beyond the active training period, and questions concerning the timing and duration of such an intervention require further study. Randomized, controlled clinical studies with objective measures of adherence can be conducted in HIV-infected subjects and should be employed for further evaluation of this and other adherence interventions.
Figures

Comment in
-
Adherence and health care utilization in HIV/AIDS-rational or rationalizing?J Gen Intern Med. 2000 Dec;15(12):891-3. doi: 10.1046/j.1525-1497.2000.01008.x. J Gen Intern Med. 2000. PMID: 11119187 Free PMC article. Review. No abstract available.
References
-
- Ioannidis JPA, Sacks HS, Cappellen JC, et al. Presented at the Fourth Conference on Retroviruses and Opportunistic Infections. Washington, DC: 1997. Clinical efficacy of antiretroviral changes in treatment-experienced HIV-infected patients: a meta-analysis.
-
- Hammer SM, Squires KE, Hughes D, et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. N Engl J Med. 1997;337:734–9. - PubMed
-
- Cameron DW, Heath-Chiozzi M, Danner S, et al. Randomized placebo-controlled trial of ritonavir in advanced HIV-1 disease. Lancet. 1998;351:543–9. - PubMed
-
- Haynes RB, McKibbon KA, Kanani R. Systematic review of randomized trials of interventions to assist patients to follow prescriptions for medications. Lancet. 1996;348:383–6. - PubMed
-
- Patterson DL, Swindels S, Mohm JA, et al. Adherence with protease inhibitor therapy for human immunodeficiency virus infections. Presented at the 38th Interscience Conference on Antimicrobial Agents and Chemotherapy. San Diego. 1998. Calif.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous