

Calcium acetate versus calcium carbonate in the control of hyperphosphatemia in hemodialysis patients
- PMID: 11120549
- PMCID: PMC11175553
- DOI: 10.1590/s1516-31802000000600006
Calcium acetate versus calcium carbonate in the control of hyperphosphatemia in hemodialysis patients
Abstract
Context: Hyperphosphatemia has an important role in the development of bone and mineral abnormalities in end-stage renal disease (ESRD).
Objective: To compare the phosphorus binding power and the hypercalcemic effect of calcium acetate and calcium carbonate in hemodialysis patients.
Type of study: Crossover, randomized, double-blind study.
Place: A private hospital dialysis center.
Participants: Fifty-two patients who were undergoing regular hemodialysis three times a week ([Ca++] dialysate = 3.5 mEq/L).
Procedures: Half of the patients were started on 5.6 g/day of calcium acetate and, after a 2 week washout period, received 6.2 g/day of calcium carbonate. The other half followed an inverse protocol.
Main measurements: Clinical interviews were conducted 3 times a week to monitor for side effects. Determinations of serum urea, calcium, phosphorus, hematocrit, Kt/V and blood gas analysis were obtained before and after each treatment.
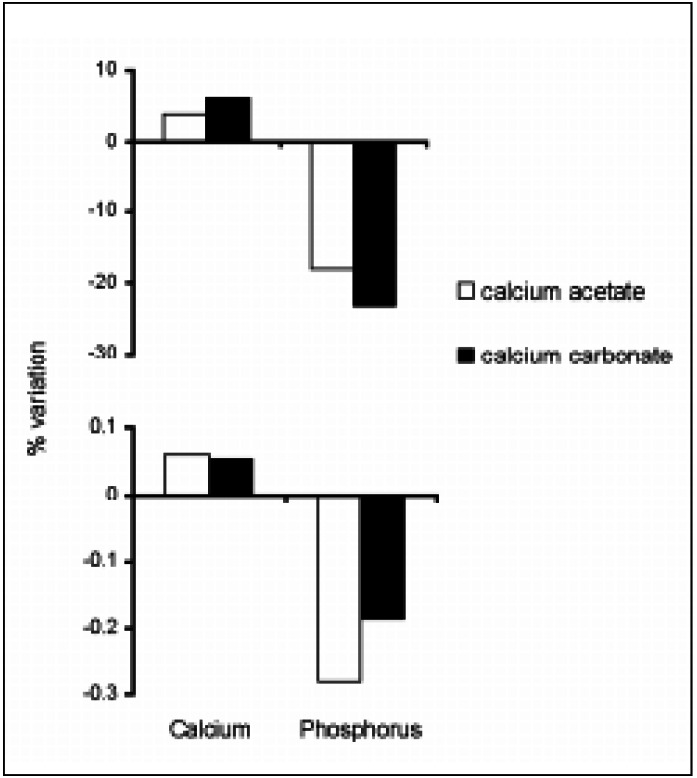
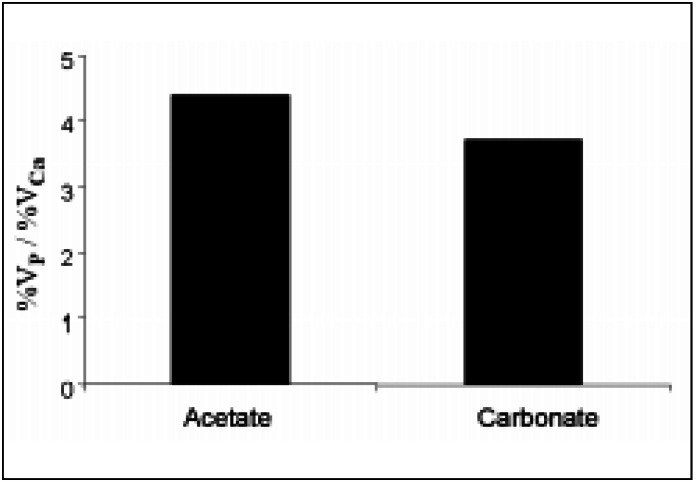
Results: Twenty-three patients completed the study. A significant increase in calcium plasma levels was only observed after treatment with calcium carbonate [9.34 mg/dl (SD 0.91) vs. 9.91 mg/dl (SD 0.79), P < 0.01]. The drop in phosphorus levels was substantial and significant for both salts [5.64 mg/dl (SD 1.54) vs. 4.60 mg/dl (SD 1.32), P < 0.01 and 5.89 mg/dl (SD 1.71) vs. 4.56 mg/dl (SD 1.57), P < 0.01, for calcium acetate and calcium carbonate respectively]. The percentage reduction in serum phosphorus (at the end of the study) per milliequivalent of salt administered per day tended to be higher with calcium acetate but statistical significance was not found.
Conclusion: Calcium acetate can be a good alternative to calcium carbonate in the handling of hyperphosphatemia in ESRD patients. When calcium acetate is used, control of hyperphosphatemia can be achieved with a lower administration of calcium, perhaps with a lower risk of hypercalcemia.
CONTEXTO:: A hiperfosfatemia tem um importante papel no desenvolvimento de anormalidades ósseas e minerais na insuficiência renal crônica terminal.
OBJETIVO:: Comparar o acetato de cálcio com o carbonato de cálcio quanto às suas propriedades quelantes de fósforo e efeitos hipercalcêmicos.
TIPO DE ESTUDO:: Ensaio clínico randomizado, cruzado, duplocego.
LOCAL:: Centro de diálise hospitalar privado.
PARTICIPANTES:: 52 pacientes em hemodiálise regular três vezes por semana ([Ca] dialisado = 3,5 mEq/l).
PROCEDIMENTOS:: Metade deles recebeu 5,6 g/dia de acetato de cálcio e, após um período de "washout" de duas semanas, 6,2 g/dia de carbonato de cálcio. A outra metade seguiu protocolo inverso.
VARIÁVEIS ESTUDADAS:: Foram conduzidas entrevistas clínicas para monitorar efeitos colaterais e obtidas amostras sangüíneas para determinações da uréia sérica, cálcio, fósforo, hematócrito, Kt/V e gasometria arterial, antes e após cada tratamento.
RESULTADOS:: 33 pacientes completaram o estudo. Um aumento significativo nos níveis plasmáticos de cálcio só foi obtido após o tratamento com carbonato de cálcio [9,34 mg/dl (SD 0,91) vs. 9,91 mg/dl (SD 0,79), P < 0,01). A queda nos níveis de fósforo foi substancial e significante para ambos os sais [5,64 mg/dl (SD 1,54) vs. 4,60 mg/dl (SD 1,32), P < 0,01 e 5,89 mg/dl (SD 1,71) vs. 4,56 mg/dl (SD 1,57), P < 0,01 para acetato de cálcio e carbonato de cálcio, respectivamente). Ao final do estudo, a redução percentual no fósforo sérico por equivalente de sal administrado por dia tendeu a ser maior com o acetato de cálcio, mas uma diferença significante estatisticamente não foi encontrada.
CONCLUSÃO:: O acetato de cálcio pode ser uma boa alternativa ao carbonato de cálcio no manejo da hiperfosfatemia em pacientes com insuficiência renal crônica terminal. Quando o acetato de cálcio é usado o controle da hiperfosfatemia pode ser alcançado com uma administração de cálcio menor, talvez acarretando um risco menor de hipercalcemia.
Conflict of interest statement
Figures
References
-
- Brent GA, LleBoff MS, Seely EW, Conlin PR, Brown EM. Relationship between the concentration rate of change of calcium and serum intact parathyroid hormone levels in normal humans. J Clin Endocrinol Metab. 1988;67:944–950. - PubMed
-
- Conlin PR, Fajtova VT, Mortensen RM, LleBoff MS, Brown EM. Hysteresis in the relationship between serum ionized calcium and intact parathyroid hormone during recovery from induced hyper and hypocalcemia in normal humans. J Clin Endocrinol Metab. 1989;320:1140–1141. - PubMed
-
- Sherwood Lm, Mayer GP, Ramberg CF, Kronfeld DS, Aubach GD, Potts JT. Regulation of parathyroid hormone secretion: proportional control by calcium, lack of effect of phosphate. Endocrinology. 1968;83:1043–1051. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
