

Acid-sensing ion channel 3 matches the acid-gated current in cardiac ischemia-sensing neurons
- PMID: 11120882
- PMCID: PMC14653
- DOI: 10.1073/pnas.98.2.711
Acid-sensing ion channel 3 matches the acid-gated current in cardiac ischemia-sensing neurons
Abstract
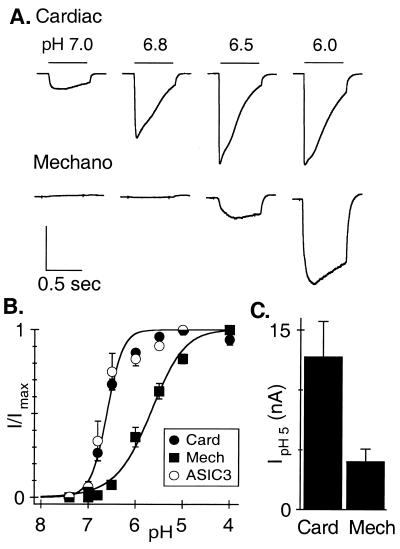
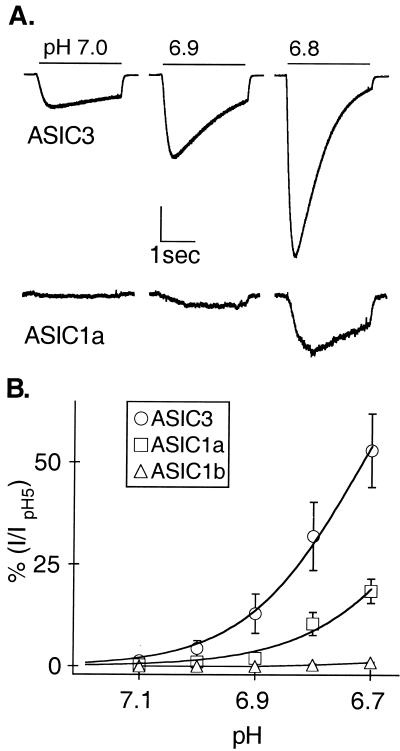
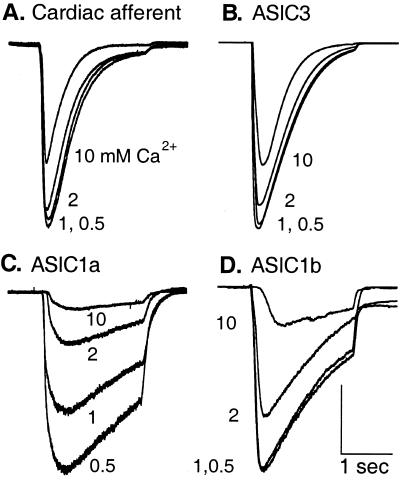
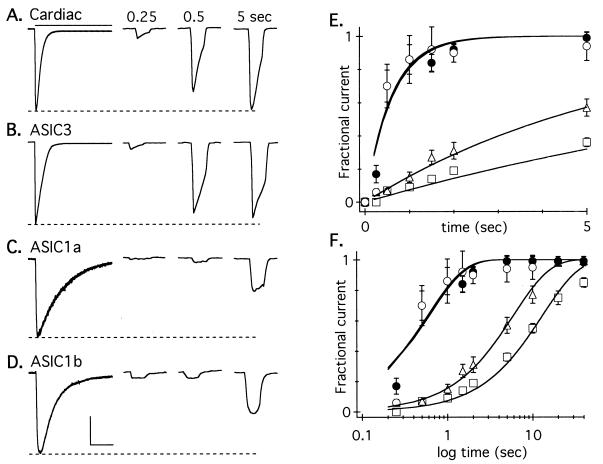
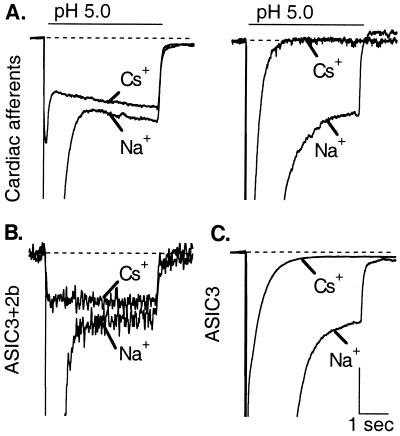
Cardiac afferents are sensory neurons that mediate angina, pain that occurs when the heart receives insufficient blood supply for its metabolic demand (ischemia). These neurons display enormous acid-evoked depolarizing currents, and they fire action potentials in response to extracellular acidification that accompanies myocardial ischemia. Here we show that acid-sensing ion channel 3 (ASIC3), but no other known acid-sensing ion channel, reproduces the functional features of the channel that underlies the large acid-evoked current in cardiac afferents. ASIC3 and the native channel are both especially sensitive to pH, interact similarly with Ca(2+), and gate rapidly between closed, open, and desensitized states. Particularly important is the ability of ASIC3 and the native channel to open at pH 7, a value reached in the first few minutes of a heart attack. The steep activation curve suggests that the channel opens when four protons bind. We propose that ASIC3, a member of the degenerin channel (of Caenorhabditis elegans)/epithelial sodium channel family of ion channels, is the sensor of myocardial acidity that triggers cardiac pain, and that it might be a useful pharmaceutical target for treating angina.
Figures
Comment in
-
Lactic acid: New roles in a new millennium.Proc Natl Acad Sci U S A. 2001 Jan 16;98(2):395-7. doi: 10.1073/pnas.98.2.395. Proc Natl Acad Sci U S A. 2001. PMID: 11209043 Free PMC article. No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
