

Long term outcome of ocular adnexal lymphoma subtyped according to the REAL classification. Revised European and American Lymphoma
- PMID: 11133714
- PMCID: PMC1723704
- DOI: 10.1136/bjo.85.1.63
Long term outcome of ocular adnexal lymphoma subtyped according to the REAL classification. Revised European and American Lymphoma
Abstract
Aim: To classify ocular adnexal lymphomas according to the Revised European and American Lymphoma (REAL) classification and to determine any correlation between clinical features or histomorphological variables with the patients' outcome.
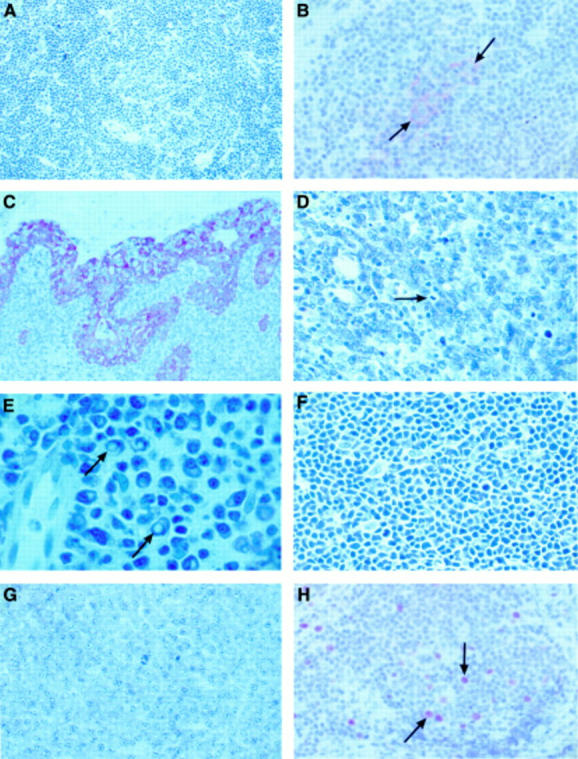
Methods: Conventional and immunohistology were performed on representative sections of 53 specimens of 46 patients with ocular adnexal lymphoma. The antibodies used were CD20, BCL-2, CD21, CD23, CD43, CD3, CD5, p53, cyclin D1, pan-cytokeratin, kappa, lambda, IgD, and IgM. The growth fraction of the tumours was determined using the MIB-1 antibody directed against the Ki-67 antigen. Clinical follow up data regarding the outcome were obtained from the treating physicians and/or hospital files. The Student's t test and log rank test were used for statistical analysis.
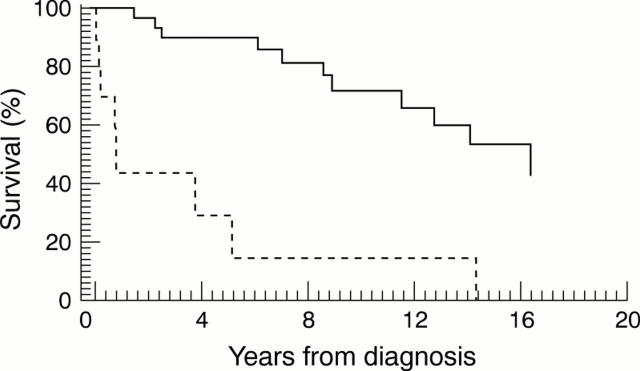
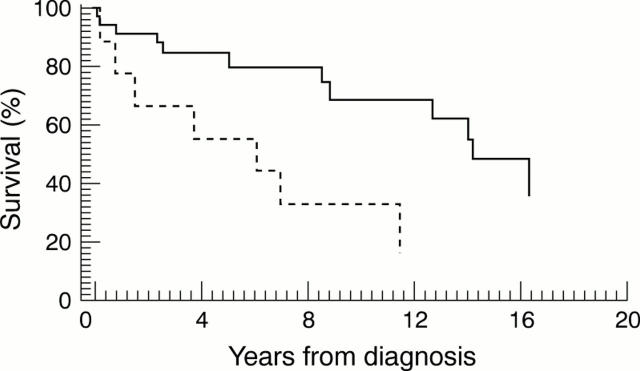
Results: The patient collective consisted of 29 females and 17 males with an age range of 32-89.7 years (average 63 years). Almost all specimens represented B cell non-Hodgkin's lymphomas: extranodal marginal zone lymphoma (EMZL) (n=38), diffuse large cell B cell lymphoma (n=8), lymphoplasmocytic lymphoma/immunocytoma (n=2), mantle cell lymphoma (n=2), follicle centre lymphoma (n=1), and plasmacytoma (n=1). One case of a secondary anaplastic large cell lymphoma of T cell type (T-ALCL) was diagnosed. The majority of the patients had stage I disease. A variety of therapeutic regimens was administered, the main form of treatment being radiotherapy. The average follow up time was 85 months. Complete remission was achieved in 24 patients (10 after excision alone, eight after radiotherapy alone, three after combined excision and radiotherapy, one after chemotherapy alone, and two after combined radiotherapy and chemotherapy). 12 patients died of causes related to lymphoma; in one patient the cause of death was unknown. Six patients had persistent tumour at final follow up and two patients were lost to follow up. The stage at presentation, as well as the lymphoma malignancy category, had a significant correlation with the final course of the disease (p=0.0001 and p=0.03, respectively). A significant correlation was also noted between the final outcome (p<0.05) and tumour cell expression for Ki-67 antigen and p53 protein.
Conclusion: 67% of patients with ocular adnexal lymphoma had EMZL. The stage at presentation had a significant influence on the final outcome. MIB-1 and p53 expression by the tumour cells proved to be important immunohistochemical markers concerning the prognosis. It is suggested that, following thorough staging investigations, primary EMZL (stage I) (if accessible) should be treated with excisional biopsy and subsequent low dose radiotherapy. Primary diffuse large cell B cell lymphoma of the ocular adnexa requires at least similar therapeutic measures and regular intensive follow up.
Figures
Similar articles
-
Outcome and prognostic factors in ocular adnexal lymphoma.Croat Med J. 2004 Jun;45(3):328-32. Croat Med J. 2004. PMID: 15185428
-
Lymphoproliferative lesions of the ocular adnexa. Analysis of 112 cases.Ophthalmology. 1998 Aug;105(8):1430-41. doi: 10.1016/S0161-6420(98)98024-1. Ophthalmology. 1998. PMID: 9709754
-
Ocular adnexal lymphomas: five case presentations and a review of the literature.Surv Ophthalmol. 2002 Sep-Oct;47(5):470-90. doi: 10.1016/s0039-6257(02)00337-5. Surv Ophthalmol. 2002. PMID: 12431695 Review.
-
T-cell and T/natural killer-cell lymphomas involving ocular and ocular adnexal tissues: a clinicopathologic, immunohistochemical, and molecular study of seven cases.Ophthalmology. 1999 Nov;106(11):2109-20. doi: 10.1016/S0161-6420(99)90492-X. Ophthalmology. 1999. PMID: 10571346
-
[Lymphoproliferative lesions of the ocular adnexa. Differential diagnostic guidelines].Ophthalmologe. 2004 Feb;101(2):197-215; quiz 216-7. doi: 10.1007/s00347-003-0854-7. Ophthalmologe. 2004. PMID: 15046030 Review. German.
Cited by
-
[Diseases of the lacrimal gland].Ophthalmologe. 2005 Apr;102(4):399-423; quiz 424-5. doi: 10.1007/s00347-005-1190-x. Ophthalmologe. 2005. PMID: 15782290 German.
-
Non‑Hodgkin's lymphomas of the lacrimal sac: Current insights and future directions (Review).Med Int (Lond). 2024 Jun 10;4(4):43. doi: 10.3892/mi.2024.167. eCollection 2024 Jul-Aug. Med Int (Lond). 2024. PMID: 38912417 Free PMC article. Review.
-
Chronic Lymphocytic Leukaemia/ Small-Cell Lymphocytic Lymphoma of the Lacrimal Sac: A Case Series.Ocul Oncol Pathol. 2017 Sep;3(3):224-228. doi: 10.1159/000455148. Epub 2017 Mar 9. Ocul Oncol Pathol. 2017. PMID: 29071273 Free PMC article.
-
Ocular adnexal lymphoma: A single-institution retrospective study.Saudi J Ophthalmol. 2022 Apr 18;35(3):230-238. doi: 10.4103/1319-4534.343368. eCollection 2021 Jul-Sep. Saudi J Ophthalmol. 2022. PMID: 35601857 Free PMC article.
-
Ocular adnexal non-Hodgkin's lymphoma: a review of epidemiology and risk factors.Expert Rev Ophthalmol. 2011 Apr;6(2):181-193. doi: 10.1586/eop.11.15. Expert Rev Ophthalmol. 2011. PMID: 23976898 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous